

Introduction
Patients under antithrombotic therapy sometimes visit our clinic for hair transplantation. Antithrombotic therapy is of critical importance to prevent serious cardiovascular events in patients with a mechanical heart valve, a coronary artery stent, or atrial fibrillation (Figure 1). Hair transplantation is considered safe surgery, therefore, peri-operative cardiovascular complications must be avoided.11-6

Mechanical Heart Valve
Thrombus formation on the metal surface of the mechanical prosthetic heart valve results in malfunction and acute regurgitation of the valve with severe heart failure, which makes the patient critically ill. A thrombosed mechanical heart valve needs to be replaced with a new mechanical heart valve, and replacement surgery is a high-risk procedure.
Peri-operative control of antithrombotic therapy is of critical importance for prevention of thrombotic events and safe surgery in patients with a mechanical heart valve (Figure 2). According to the most recent guidelines, antithrombotic drugs should not be stopped and should be continued in a reduced dose before surgery.

Bridging Anticoagulation
The author doesn’t stop warfarin before surgery in patients with a mechanical heart valve. Some cardiologists and other physicians may recommend stopping warfarin and antiplatelet drugs for one week before surgery. Because it is written in many books, sometimes cardiologists recommend bridging antithrombotic therapy using low molecular weight heparin.
This heparin-bridging regimen is one of incorrect information in modern medicine, and it should not be recommended. There is no evidence based on scientific data for heparin bridging. For more than 30 years, basic scientists have pointed out that heparin doesn’t prevent platelet activation and coagulation cascade. Heparin doesn’t stop the thrombotic process, even though heparin seems to prevent blood clot formation. A few years ago the American Heart Association and the American College of Cardiology Foundation (AHA/ACCF) published a guideline stating that the societies don’t recommend the heparin bridging regimen anymore.1,3-5 Several studies show that heparin doesn’t prevent arterial thromboembolic events whereas heparin increases the risk of major bleeding.2,6 There are many physicians and cardiologists who don’t know the new guideline and still recommend heparin bridging for patients under antithrombotic therapy.
Safe Guide on Peri-operative Control of Warfarin
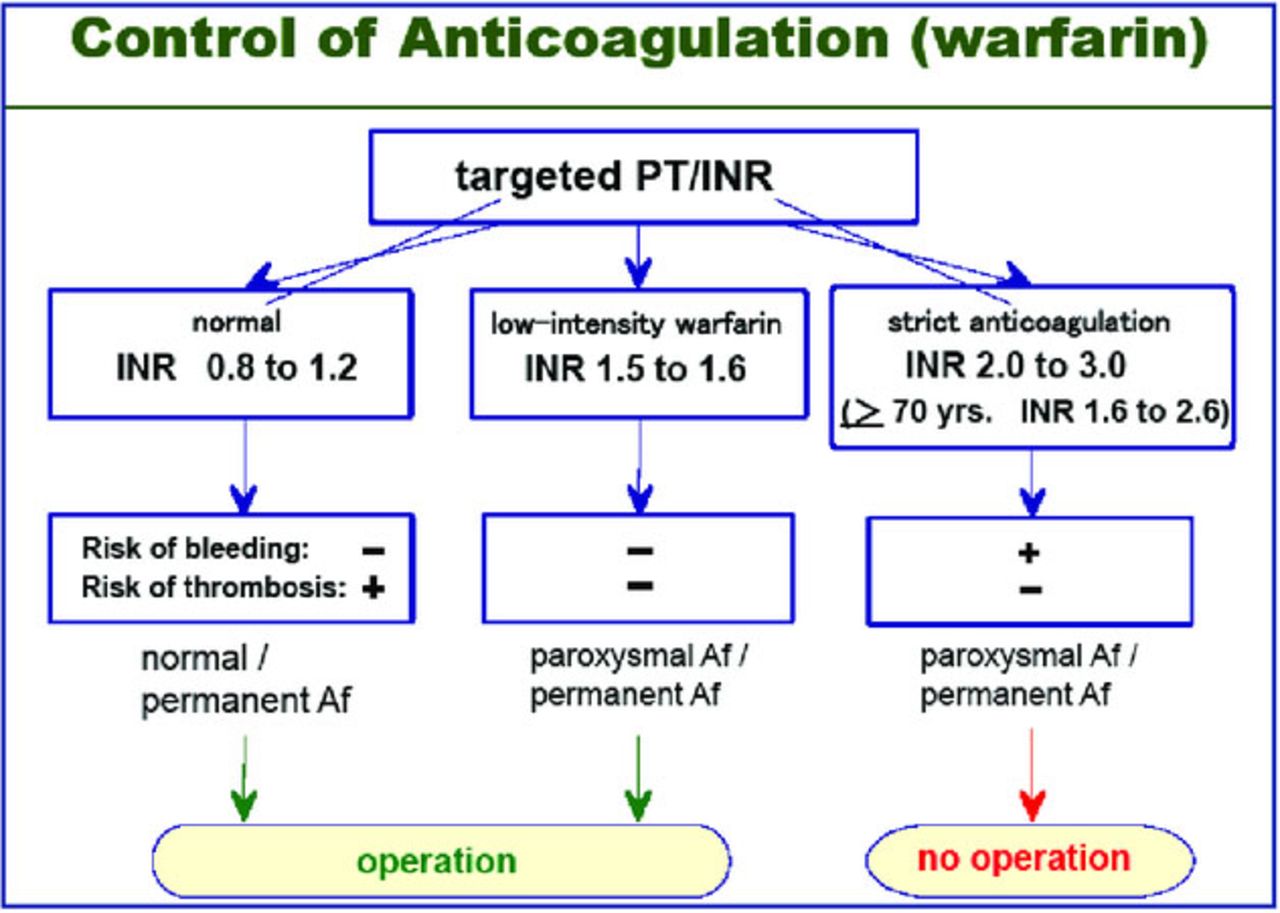
Warfarin (Coumadin) is slow-acting and has a long half-life. The half-life of warfarin is about 36 hours in the blood. The anticoagulant effect of warfarin appears in 12-24 hours and lasts for 48-72 hours. In the clinical experience, warfarin remains effective for 3-4 days after it is stopped, and it takes 4-5 days for warfarin to reach the therapeutic effect after it is restarted. The anticoagulant activity of warfarin is closely monitored by the prothrombin time/international normalized ratio (PT/INR) to ensure that an adequate and safe dose is taken.7 The targeted PT/INR level tends to be 2.0-3.0 in most conditions as maintenance anticoagulant therapy for the prevention of thrombosis in patients with mechanical heart valves.
If the PT/INR is 2.0-3.0, the patient has a risk of bleeding but there is little risk of thrombosis.8 This strict anticoagulation is applied to patients with a mechanical heart valve or atrial fibrillation. A PT/INR of 0.8-1.2 is normal coagulability, and there is little risk of bleeding but there is a risk of thrombosis. If the PT/INR is around 1.5-1.6, there is little risk of bleeding or thrombosis. This means low-intensity anticoagulation can be applied for less than one week to a patient with a mechanical heart valve and paroxysmal atrial fibrillation (Figure 3).

Interruption of anticoagulation before surgery can be problematic. If warfarin is stopped for longer than 4-5 days pre-operatively, the PT/INR will return to normal (<1.2) on the day of the procedure, and the patient will remain unprotected for about 3-4 days post-operatively. The period off warfarin can be shortened by restarting warfarin in the maintenance dose one day before the procedure with the expectation that coagulability will become nearly normal on the day of the procedure and warfarin will become effective again soon after the surgery.
If warfarin is stopped, there is a risk of thrombosis in patients with a mechanical heart valve. Therefore, the dose of warfarin should be reduced gradually 5-6 days before surgery. The final dose of warfarin can be reduced to two-thirds to three-fourths of the maintenance dose for 2-3 days before surgery to allow the PT/INR to fall to around 1.5-1.6 on the day of the surgery. If the PT/INR is around 1.5 on the day of the procedure, warfarin will not cause hemorrhagic tendency or thrombus formation. This low-intensity warfarin doesn’t interfere with surgical procedures including abdominal surgery, orthopedic surgery, cardiac surgery, and tooth extraction. Hair transplantation can be performed without any difficulty. Further reduction of the dose of warfarin is dangerous and not necessary. Warfarin should be restarted in the maintenance dose soon after the surgery. Warfarin should not be stopped before hair transplantation in patients at high risk of thrombosis (Figure 1).
Safe Period with Low-Intensity Warfarin
At the outpatient clinic, the result of PT/INR varies often according to a patient’s dietary habits. If the patient takes antiplatelet drugs, the patient is safe even if the PT/INR is kept around 1.4-1.6 for several weeks or one month. If the patient takes no antiplatelet drugs, the period of PT/INR of 1.5-1.6 should be kept short and the period off warfarin should be less than a few days.
Aortic Valve vs. Mitral Valve
As for the difference in the location of the mechanical heart valve, a prosthetic heart valve at the aortic position has less possibility to form thrombus than one at the mitral position because of high blood velocity and high driving pressure to open and close the valve. Patients after aortic valve replacement have less possibility of thrombosed valve than those after mitral valve replacement, even when they are kept under insufficient antithrombotic therapy for a few months.
Prosthetic heart valves at the tricuspid and pulmonary positions are more likely to form thrombus because of slow blood flow and low driving pressure to open and close the valve. This is the reason why mechanical heart valves are not used at the tricuspid and pulmonary position.
In addition, there is an increased risk of thrombosis of a mechanical heart valve if the patient receives poor control of antithrombotic therapy for several months.
Antiplatelet Drugs
Patients with a mechanical heart valve need a combination of anticoagulant and antiplatelet drugs to prevent clot formation and growth.8 Dipyridamole and ticlopidine are usually used as antiplatelet drugs for mechanical heart valves. Dipyridamole has a moderate antiplatelet effect. Ticlopidine is a relatively strong antiplatelet drug.
About 30-40 years ago, only an anticoagulant without antiplatelet drugs was prescribed for patients after valve replacement, and thrombosed mechanical heart valve was not rare in those days.
Antiplatelet drugs should only be stopped for a short period in patients with a mechanical heart valve. The length of time without antiplatelet drugs is determined by the half-life and irreversibility of the drug.8 The half-life of dipyridamole is short and the effect is reversible, and dipyridamole can be stopped only 1-2 days before surgery. If the antiplatelet drug has a long half-life and irreversible effect, it needs to be stopped 3-7 days before surgery. Ticlopidine can be stopped 5-7 days before surgery, but not longer than one week. It is also important to restart the antiplatelet drugs in the maintenance dose on the first day following the surgery.
Aspirin is a weak antiplatelet drug, and aspirin is not enough for antithrombotic therapy in patients with a mechanical heart valve. Usually, aspirin is not used as an antiplatelet drug in patients with a mechanical heart valve. If a patient does take aspirin as an antiplatelet drug, aspirin can be continued for surgery. Low-dose aspirin doesn’t cause hemorrhagic tendency during the surgery.
Patients with a Mechanical Heart Valve
Over 30 years of practice, this author has treated hundreds of patients with mechanical heart valves in an outpatient clinic. Patients with a mechanical prosthetic valve need lifelong antithrombotic therapy using a combination of warfarin and antiplatelet drugs.8 As these patients aged, some needed various kinds of operations including major surgery such as cholecystectomy for gallstones, colectomy for colon cancer, knee joint replacement, another heart valve replacement, coronary artery bypass graft surgery, etc. Patients sometimes also needed minor surgery such as tooth extraction, cataract operation, skin cancer removal, and empyema operation in the nasal cavity. All the patients went through these procedures safely without a thrombotic event when managed as outlined above.
As for the duration of hair transplantation, there is enough time to operate on the patient as usual. It is not necessary to hurry to finish the operation. If the drugs are controlled properly before surgery, patients remain safe for several days with a reduced dose of antithrombotic drugs.
Coronary Artery Stent
Stent thrombosis is a serious complication.9,10 Thrombus in the coronary stent occludes the lumen of the stent, which results in acute myocardial infarction. Stent thrombosis is a life-threatening complication with a high mortality rate of 20%. Antiplatelet drugs are necessary to prevent thrombus formation in coronary artery stents. Patients with coronary artery stents need long-term antiplatelet therapy (Figure 2).
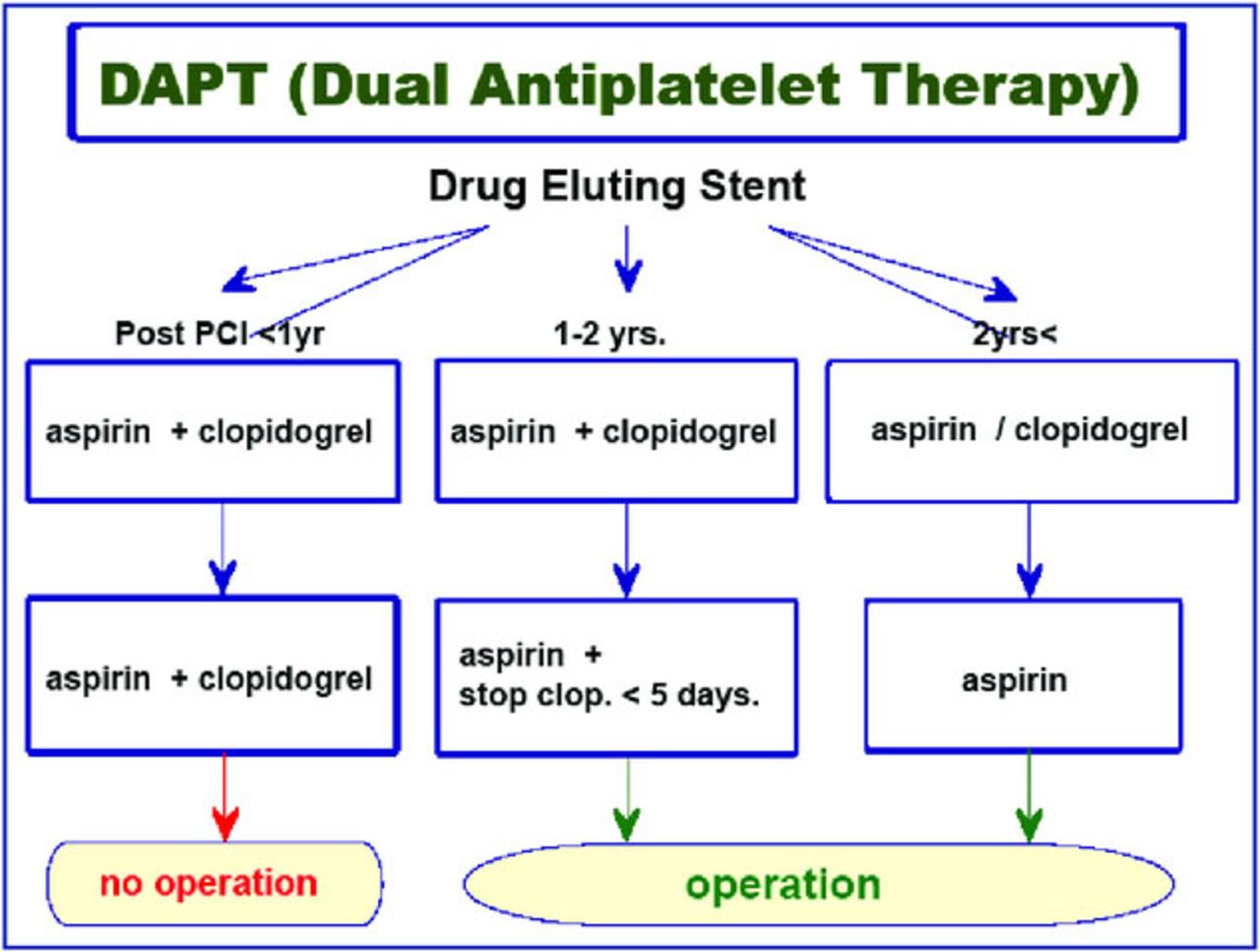
Drug eluting stents are usually selected for percutaneous coronary intervention. Antithrombotic therapy for patients with drug eluting stents is as follows (Figure 4). Patients within one year after the coronary intervention using drug eluting stents need a combination of two antiplatelet drugs. This dual antiplatelet therapy (DAPT) means the combination of aspirin 81mg per day (ranging 75-100mg) and another stronger antiplatelet drug such as a P2Y12 inhibitor (clopidogrel, prasugrel, or ticagrelor). Aspirin is always continued in patients with coronary artery disease regardless of the duration of DAPT.

DAPT
DAPT is used to reduce the risks of future heart attack and coronary stent thrombosis, which means occlusion of a stent by a blood clot. In general, DAPT cannot be stopped for one year. Hair transplantation should be postponed until one year after the stenting treatment.
In patients from one to two years after stenting treatment using drug eluting stents, hair transplantation is possible. Patients usually need both aspirin and clopidogrel in this period. Clopidogrel can be stopped for 5 days as long as aspirin is continued, and safe hair transplantation is possible as usual in these patients (Figure 4). If you want to stop both drugs, you can stop them for only 3 days before surgery but not longer. After hair transplantation, however, both drugs should be restarted.
In patients more than two years after stent implantation using a drug eluting stent, one antiplatelet drug is used in the long term. If the patient takes clopidogrel, it can be changed to aspirin for one week before surgery, and then the clopidogrel can be restarted after the hair transplantation. If the patient takes aspirin as an antiplatelet drug, it can be continued before surgery (Figure 4). Safe hair transplantation is possible as usual with a maintenance dose of aspirin. Even FUE is possible in patients with low-dose aspirin because low-dose aspirin doesn’t cause hemorrhagic tendency during surgery. Aspirin should be stopped for no more than 3-5 days.
This year, the American College of Cardiology Foundation (ACCF) and the American Heart Association (AHA) released updated guidelines for dual antiplatelet therapy in patients with a coronary artery stent.11 The new guidelines are based on the findings of recent studies in patients with a new type of stents that lowers the risk of clotting complication better than the older types of coronary stents. The updated recommendations on duration of DAPT compiled six previously published guidelines, which were published by the ACCF/AHA from 2011 to 2014. The new guidelines recommend a shorter duration of DAPT (short DAPT) in patients with a low risk of stent thrombosis and a high risk of bleeding. The guidelines also recommend a longer period of DAPT (long DAPT) in patients with a high risk of stent thrombosis and a low risk of bleeding. In general, DAPT for 6-12 months is a Class I recommendation, and DAPT for more than 12 months is a Class IIb recommendation. These recommendations apply to a new generation of coronary stents with less possibility of stent thrombosis and to patients without oral anticoagulant therapy.
Maintenance drugs should be checked in patients with a coronary artery stent. If the patient needs antiplatelet drugs as maintenance therapy, it is important to talk to the patient’s physician about these drugs. If the cardiologist doesn’t mind stopping the antiplatelet drugs for several days, antiplatelet drugs can be stopped before surgery and restarted after the surgery. If the cardiologist doesn’t allow the antiplatelet drugs to be stopped, the drugs should be continued before the procedure. Hair transplantation is an operation with low risk of bleeding. Safe operation is possible even in patients using low-dose antiplatelet drugs.
Risk of Cardiovascular Event
It is important to compare the risk of bleeding and the risk of thrombosis in cardiovascular patients (Figures 1 and 5). Patients with a coronary artery stent and unstable angina pectoris belong to a high-risk group. In these patients, thrombosis may cause serious cardiovascular events and acute myocardial infarction. Antithrombotic drugs should be continued in the maintenance dose or they can be reduced to two-thirds dose for only a few days before the hair transplantation. If antithrombotic drugs are stopped before surgery, the patient will be put at risk for thrombosis with high mortality.

If a patient needs clopidogrel as antithrombotic therapy, there are two possibilities. First, ask the cardiologist if clopidogrel can be switched to low-dose aspirin for one week. If the cardiologist agrees with low-dose aspirin, it can be continued and a safe hair transplantation without difficulty in hemostasis can be performed. Second, if the cardiologist doesn’t agree with aspirin, ask if the dose of clopidogrel can be reduced to one-half to two-thirds of the maintenance dose. If the dose of clopidogrel can be reduced before surgery, the hair transplantation can be performed without major difficulty. If the cardiologist doesn’t agree with dose reduction of clopidogrel, the hair transplantation should be performed carefully, or the operation postponed for one year. After one year, the cardiologist will probably agree with dose reduction or change of the drug.
Atrial Fibrillation
Loss of wall contraction and stasis of blood flow tend to cause thrombus formation in the left atrial appendage in patients with atrial fibrillation.12-17 Thrombus in the left atrial appendage is usually large in size, and thromboembolism of the clot occludes the large artery in the cranium. Symptoms of large vessel embolic ischemic stroke include hemiplegia, speech disturbance, etc.
An anticoagulant drug prevents clot formation in the left atrium (Figures 1-3). Warfarin is used to prevent ischemic stroke in patients with atrial fibrillation. Targeted maintenance anticoagulation of warfarin is usually a PT/INR of 1.6-2.6 in patients with atrial fibrillation.
Patients with paroxysmal atrial fibrillation have a high risk of thrombosis if warfarin is discontinued; rather, warfarin should be reduced to two-thirds of the maintenance dose for 4-5 days in advance of surgery to allow the PT/INR to fall to near normal (1.4-1.6) (Figure 3). The maintenance dose of warfarin should be resumed post-operatively.
Patients with permanent atrial fibrillation have a low risk of thrombosis, and warfarin can be stopped or reduced to half of the maintenance dose for 5-7 days before surgery to allow the PT/INR to fall to normal or near normal (1.0-1.5). The maintenance dose of warfarin should be restarted after surgery.
If the PT/INR is around 1.5-1.6, there is little risk of bleeding or thrombosis. This means low-intensity anticoagulation can be safely prescribed for less than one week for patients with paroxysmal or permanent atrial fibrillation.
NOAC
Recently, several new anticoagulants (novel oral anticoagulants [NOAC]) have become commercially available. They are direct thrombin inhibitors. Their bioavailability is not affected by foods, and similar effective results are expected without blood tests. The half-life of dabigatran is 12-14 hours, the half-life of apixaban is 9-14 hours, rivaroxaban 7-11 hours, and edoxaban 9-11 hours. Dabigatran is a direct thrombin inhibitor. Apixaban, rivaroxaban, and edoxaban are selective direct inhibitors of clotting factor Xa. The dosage of NOAC is reduced to two-thirds or one-half per day to avoid bleeding complication in patients over 70-80 years of age or in patients with moderately impaired renal function. If NOAC is stopped for 24 hours before surgery, coagulability will return to nearly normal on the day of the procedure. Major surgery is possible if NOAC is stopped for 2 days before surgery.
NOAC is usually recommended as antithrombotic therapy in patients with atrial fibrillation. NOAC reduces the risks of stroke, systemic thromboembolism, and major bleeding in comparison with warfarin. However, if a major bleeding complication happens, the patient’s condition may become serious and sometimes be fatal. There are several recent reports on fatal intracranial bleeding in elderly patients under antithrombotic therapy using NOAC. There is no laboratory measure for the effect of NOAC, or to determine when NOAC is overdosed. Currently, there is also no drug to counteract the effect of NOAC when the patient has bleeding complications. Therefore, NOAC should be used carefully and only by experienced cardiologists.
Risk of Bleeding vs. Risk of Thrombosis
It is important to compare the risk of bleeding and the risk of thrombotic events in patients under antithrombotic therapy (Figure 5). Diseases that require lifelong antithrombotic therapy are classified into either 1) a low-risk group or 2) a high-risk group (Figure 1).
Disorders in the high-risk group include unstable angina pectoris, recent cerebral infarction, paroxysmal atrial fibrillation, and patients with mechanical prosthetic heart valve and coronary artery stents. Thrombosis may cause serious cardiovascular events in these patients, and antithrombotic drugs should not be stopped before hair transplantation.
Disorders in the low-risk group include old myocardial infarction, old cerebral infarction, permanent atrial fibrillation, bioprosthetic heart valve, deep vein thrombosis, and pulmonary embolism. Thrombosis does not directly cause serious cardiovascular events in these patients, and antithrombotic drugs can be stopped only for a short period before surgery.
Antithrombotic Therapy
Antithrombotic therapy consists of anticoagulant and antiplatelet drugs (Figure 2). Anticoagulant drugs reduce fibrin formation and slow down clotting. Antiplatelet drugs prevent platelets aggregation. A combination of anticoagulant and antiplatelet drugs is important to prevent clot formation and growth.
An anticoagulant drug prevents thrombus formation in slow blood flow, where an antiplatelet drug has little effect. An anticoagulant is effective to prevent thrombus formation in the left atrial appendage in atrial fibrillation, deep vein thrombosis, venous thromboembolism, etc.
An antiplatelet drug prevents thrombus in the arterial circulation with fast blood flow, where an anticoagulant is not effective. Antiplatelet drugs prevent thrombosis in the coronary artery stent, and in many cerebrovascular and cardiovascular diseases.
Patients with a mechanical heart valve need both anticoagulant and antiplatelet drugs to prevent thrombosis. Only an anticoagulant drug or only an antiplatelet drug is not enough to prevent thrombosis on the mechanical heart valve.
Other Issues in Cardiovascular Patients
There are other considerations for safe surgery in elderly patients and patients with cardiovascular diseases.
Beta Blocker
Patients with cardiovascular diseases sometimes need a beta blocker as one of maintenance drugs for the treatment of hypertension, heart failure, and tachyarrhythmia.18,19 Usually, a beta-1 selective blocker such as bisoprolol, atenolol, or metoprolol is used (Table 1). A beta blocker works effectively to control hypertension and tachyarrhythmia including paroxysmal atrial fibrillation. If a patient takes a beta blocker for cardiovascular diseases, it is not a good idea to stop the beta blocker before hair transplantation. If a beta blocker is stopped before surgery, there is the possibility that the patient will have uncontrollable hypertension or dangerous tachyarrhythmia during surgery.
There is a guideline on peri-operative usage of beta blockers published by the American Heart Association/American College of Cardiology Foundation (AHA/ACCF) that recommends continuation of a beta blocker before non-cardiac vascular surgery. If the patient needs a beta blocker for the treatment of tachyarrhythmia, hypertension, and other cardiovascular diseases, a maintenance dose of beta blocker should not be stopped before surgery. Peri-operative beta blockade in cardiovascular patients is a Class I indication on the level of evidence B or C in the ACCF/AHA guidelines. Safe operation is possible as usual even when a small dose of epinephrine is added in the tumescent solution. A beta-1 selective blocker reduces peri-operative mortality and non-fatal heart attacks in patients undergoing non-cardiac vascular surgery. A beta blocker should be continued before hair transplantation in patients with cardiovascular diseases.
Beta Blocker
Epinephrine
This author usually dilutes epinephrine in the concentration of 1:500,000 to 1:1,000,000 in the tumescence. The concentration is enough for vasoconstriction and hemostasis. The author prefers intradermal injection of tumescent solution all around the recipient area and the donor area. Most of the blood flow comes through the dermal layer, and there is little blood supply from the subcutaneous adipose tissue. This author usually has difficulty finding slits in the recipient area, because only a little bleeding can be seen during surgery. Over the past 10 years, this author has never used “super juice” with high epinephrine concentration during surgery.
Hair transplant surgeons are sometimes afraid of bleeding from slits, and they want to stop antiplatelet drugs and anticoagulants before surgery. However, bleeding from slits and antithrombotic drugs are different issues. Bleeding from slits can be reduced by intradermal injection of tumescent solution containing a small dose of epinephrine all around the recipient area. If bleeding from a slit is caused by injury of an intradermal vessel, an additional intradermal injection of tumescent solution at the site of bleeding can be given. Increased tissue pressure minimizes bleeding from the slit; gauze can be used to compress the slit for a few minutes while making slits in other places in the recipient area. Subcutaneous injection of super juice has little effect on bleeding from slits.
Others
In at-risk patients, electrocardiogram, blood pressure, heart rate, and peripheral oxygen saturation (SpO2) should be monitored throughout surgery.
This author always uses nitroglycerin (NTG) tape in patients with ischemic heart disease or patients older than 60 years of age. A half size of 5mg NTG tape is put on the anterior chest wall of the patient 15-20 minutes before surgery. It will keep a stable subtherapeutic concentration of NTG in the blood during surgery, which will make the operation safer. When the tape is removed, the effect of NTG will disappear. Usage of a small dose of NTG has no side effect.
Sedative drugs will be helpful to reduce anxiety and sympathetic nerve activity in patients with ischemic heart disease and tachyarrhythmia. Painkillers also can be helpful during operation. The author prefers fentanyl tape to reduce pain during and after surgery. A half size of 1mg fentanyl tape works satisfactorily.
Nasal oxygen 1.5-2L/min should be prepared to avoid hypoxemia during surgery. It is safer to keep SpO2 of 96-98% or greater during surgery.
An intravenous cannula should be inserted before surgery in cardiovascular patients And an anesthesiologist should be there to help during the surgery. In addition, 500-1,500cc Lactated Ringer’s solution should be prepared for volume replacement in case of hypotension and hypovolemia. Drinking isotonic sports drinks is also useful as volume replacement before surgery.
Hypotension should be avoided during surgery in patients with ischemic heart disease.20 If the systolic arterial pressure drops to less than 90mmHg during surgery, the patient’s lower legs should be raised and the patient should be put in Trendelenburg position. If the systolic arterial pressure drops below 80mmHg, the patient with ischemic heart disease will be at risk of cardiac arrest and should be given transfusion and vasopressor. The author gives the patient rapid transfusion of 1,000-1,500cc Lactated Ringer’s solution and an intravenous injection of ephedrine. Ephedrine is effective to treat low arterial pressure during surgery. Intravenous injection of 4-6mg ephedrine can be repeated every several minutes up to 2-3 times. After an injection of a total of 12-16mg ephedrine, the systolic arterial pressure should become greater than 90-100mmHg again, and the operation can be restarted. Ephedrine is a safe and effective vasopressor to treat low systolic arterial pressure during surgery.
Conclusion
Over a 10-year period, the author has performed 48 hair transplantation surgeries in 26 male patients with cardiovascular and cerebrovascular diseases. Patients needed maintenance antithrombotic therapy in 26 operations. They included ischemic heart disease in 11, ischemic cerebral disease in 8, atrial fibrillation in 4, prosthetic heart valve in 2, and pulmonary embolism in 1. All these patients underwent safe surgery without complications. The author always continued beta blocker, anticoagulant, and antiplatelet drugs before surgery, which made the hair transplantation safer.
A note from Dr. True: One of the greatest strengths of our Society is the diversity of backgrounds of our membership. Because of our primary specialties, many of us bring unique expertise to our Society—neurosurgery, urology, facial plastics, dermatology, cardiology, ENT, anesthesiology, etc. And when our members share insights from their background, it often enhances all of our practices. The lead article in this issue is a perfect example. Our immediate Past President, Dr. Kuniyoshi Yagyu, is a cardiologist by training. He has contributed many articles and presentations on the management of cardiology conditions during hair restoration surgery and in this issue he offers a very thorough and clearly written guide to help us provide correct peri-operative management of antithrombotics in hair transplantation.
I also would like to express Dr. Mario Marzola’s and my gratitude on behalf of all the members to Dr. Yagyu for his outstanding leadership of our Society. We have been fortunate to have had the right leader at the right time to guide us through some difficult issues. We should hope that other societies and nations will be fortunate to have leaders of the same quality.
On page 252, we share an excerpt from Dr. Yagyu’s opening remarks at the 24th ISHRS World Congress just concluded in Las Vegas.
Excerpt from Dr. Kuniyoshi Yagyu’s Opening Remarks from the 24th ISHRS World Congress

The ISHRS is against misleading advertisements. False advertisement should not be made by the ISHRS members. The words “No Scar” in the donor area and “No Pain” procedure should not be used in the advertisement or on the website. Medical advertising must adhere to the truth. Physicians are required to adhere to high ethical standards, because you are proud members of the ISHRS.
The ISHRS is a society where surgeons perform the surgery. The ISHRS is not a society where non-licensed technicians perform surgery. Qualified physicians make all surgical incisions of FUE and FUT. All decisions during the surgery should be made by physicians. Hair transplantation procedure should be performed by physicians. A non-licensed person is not allowed to perform hair transplantation surgery.
Hair restoration is usually a safe procedure. However, problematic situations do develop from time-to-time. Sometimes a fatal complication has been reported even in young patients. Problematic situations may be encountered during surgery. We should always be prepared for possible complications.
The simple rule of doing no harm is not enough. We should always try to do the right thing for the patient. The patient must be served well.
The ISHRS is strongly against the paradigm that allows technicians to perform hair transplantation surgery. The Society has been struggling to achieve this hard task for many years. We had many difficulties in attaining our objective. Recently, we took a step forward in some countries and states. There are still many difficulties in the legislative lobbying efforts but we keep our energy and passion to move forward to protect our patients. Patients’ safety is upmost importance for the Society. The ISHRS is the society where physicians perform the surgery. We are against a non-licensed practice of medicine.
I trust you. I trust our members. We unite everybody, which gives us the power. We leave no one behind. This is the direction for our Society.
Ladies and gentlemen, members of the Society, today, if you have the same thoughts that I do, if you have the same hope that I do, if you have the same energy that I do, if you feel the same urgency that I do, if you feel the same passion that I do, if we do what we must do, then I have no doubt that all the patients in the world, from east to west, from south to north, will be happy.
Patients will enjoy safe surgery with ethics. We promote science in the hair restoration surgery. All physicians unite once again under the flag of the ISHRS. And the ISHRS will achieve the mission.
After the long hard days, a bright day will come.
- Copyright © 2016 by The International Society of Hair Restoration Surgery
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.