

- Kapil Dua, MBBS, MS
- Aman Dua, MBBS, MD
- Renu Kothottil, MBBS, MD
Beards are great for rubbing when deep in thought, they block the sun from burning your face, they hide neck flab, and they suggest a life free from razor burn. And while some men have thick growth of facial hair, others may not, due to a variety of reasons, and yearn to have it. With more and more people knowing about the possibility of the beard and moustache reconstruction, many are now undergoing transplant in these areas, and they can have different facial hairstyles.
This trend of the growing popularity of facial hair restoration is also catching up with ISHRS members. As was reported in the ISHRS 2013 Practice Census, about 7% of hair transplant surgeries were performed for non-scalp areas, out of which more than 90% were to the facial area.1 This included restoration of eyebrows, eyelashes, beard, and moustache. At our clinic, the trend is similar in that facial hair transplant constitutes about 5% of our total surgeries. The majority of our facial hair cases are beard and moustache restoration; the remainder are eyebrows (Figure 1).
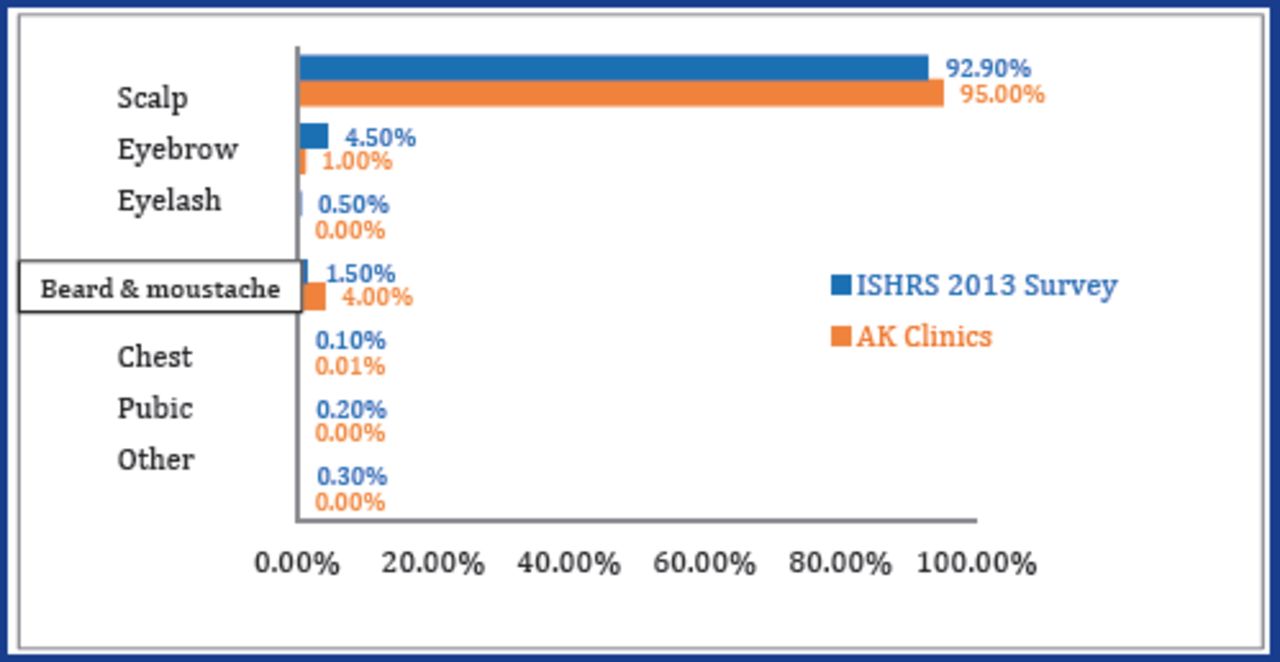
Frequency of hair transplant procedures by body area
This article shares our experience on the reconstruction of the beard and moustache.
Why do patients undergo moustache and beard transplant?
There are a variety of reasons patients choose this type of transplant, and many suffer from the following:
Scars due to trauma, burns, or surgery (Figure 2)
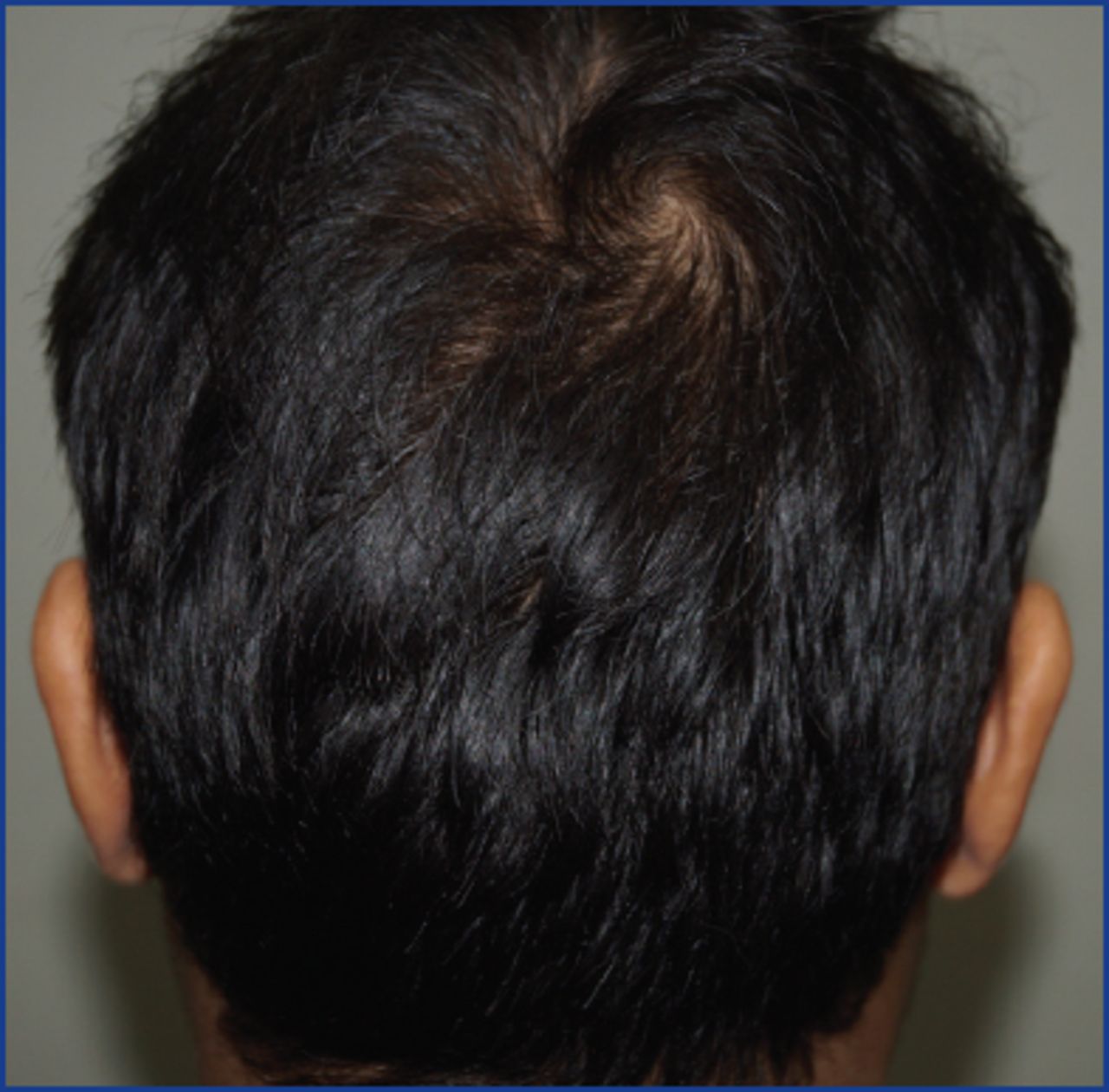
Traction alopecia (especially in Indian Sikh population) (Figure 3)
Congenital hypotrichia/atrichia (Figure 4)
Post-folliculitis scarring
Long-standing alopecia areata

Burn scar

Traction alopecia

Congenital hypotrichia
In addition, many men simply want to improve the density in certain areas of their beard or moustache depending on certain styles they would like.
Is it any different from the routine scalp hair transplant?
Yes, it is slightly different from scalp hair transplantation. But before going into the details of the procedure, it is imperative to review the anatomy of the beard and the difference between the characteristics of the scalp and beard hair.
Beard and moustache hairs consist of mainly single-hair follicular units. The beard growth starts during puberty, under the influence of androgens, and increases in density until the mid-30s. This is in contrast to the scalp, where the increased action of androgens causes hair loss.2
There are differences among different ethnic groups. Indian and Middle Eastern men have denser beards.3 Caucasians and Africans also have good density; they have more hair in the beard compared to Orientals.4
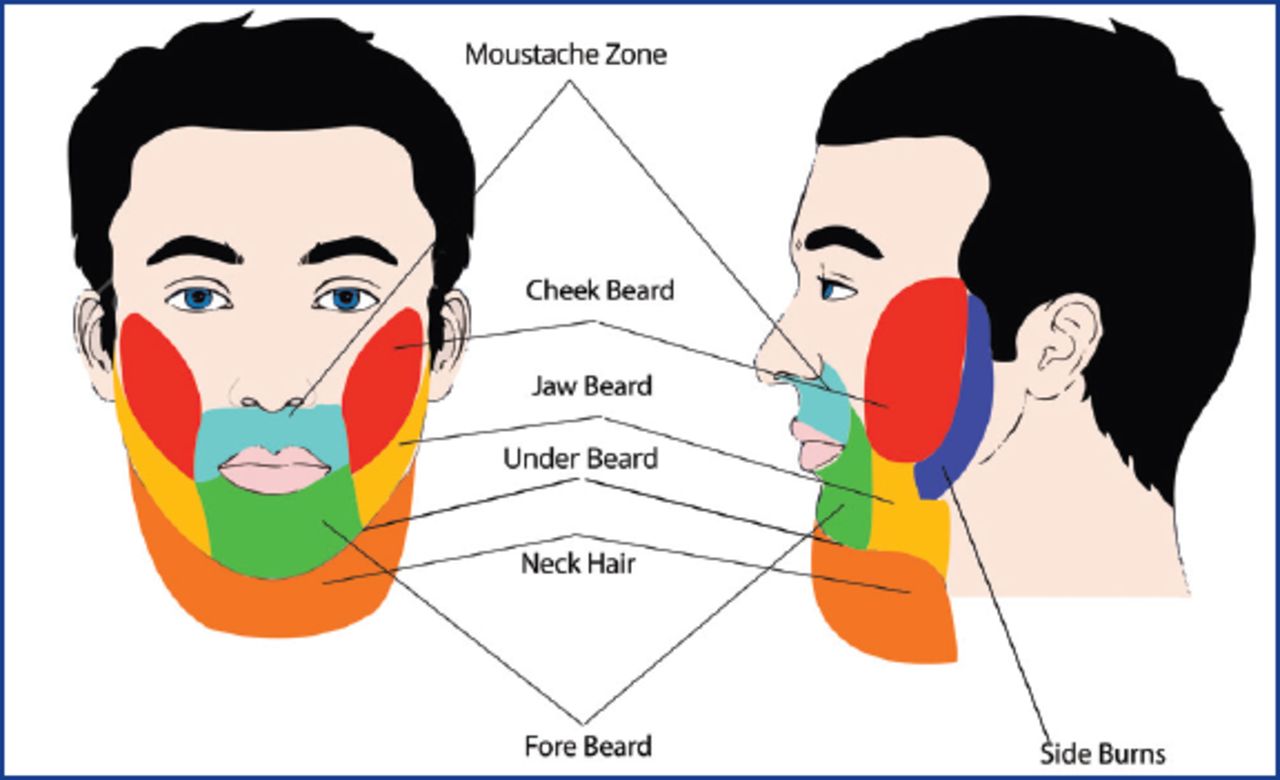
For the purpose of facial reconstruction, we divide the face into lateral and frontal aspects (Figure 5). The lateral aspect includes the sideburns, the cheek beard, the jawline beard, and the submandibular beard area. Out of these four areas, the cheek beard is cosmetically the most important. In the frontal aspect, the fore beard, comprised of the mustache and goatee (chin and sublabial beard), is the prominent feature and higher densities are present in this area. In its pure definition, the goatee does not include the moustache. The hair below the chin and jawline that extends onto the neck is also usually considered to be part of the beard.
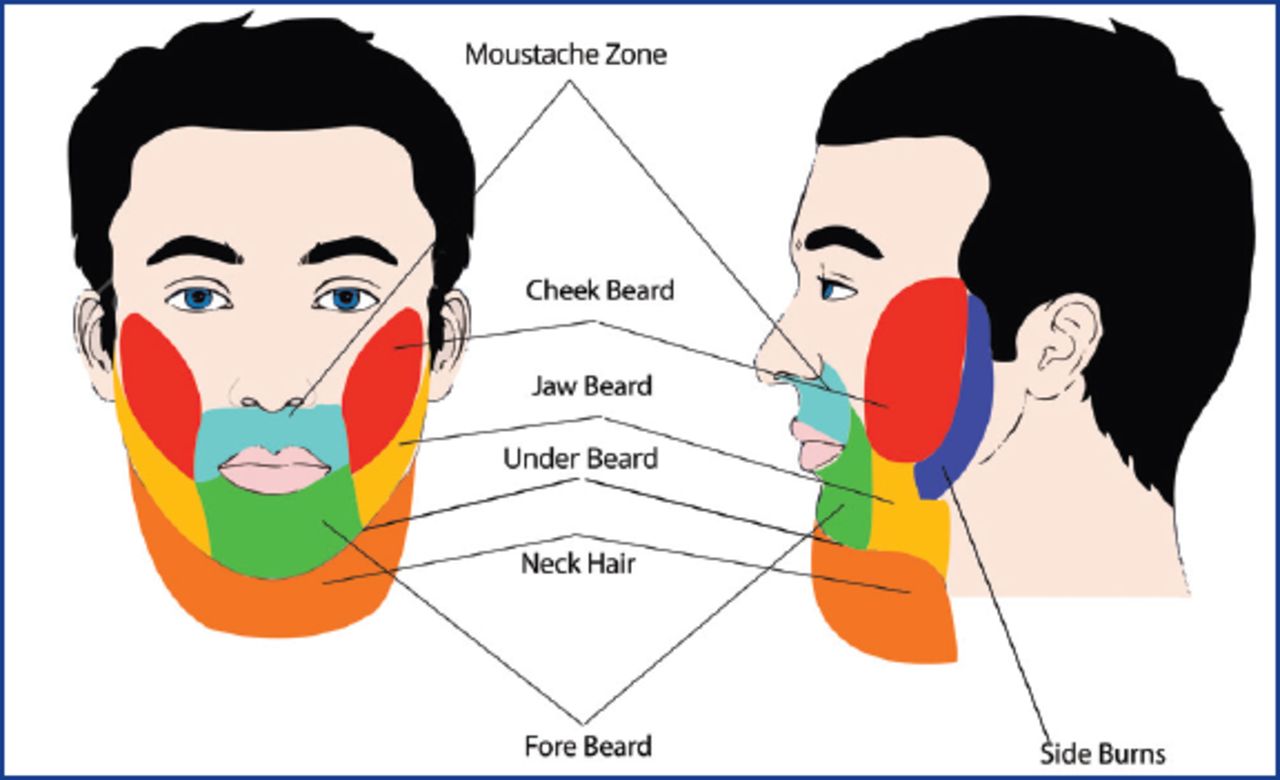
Anatomy of the beard
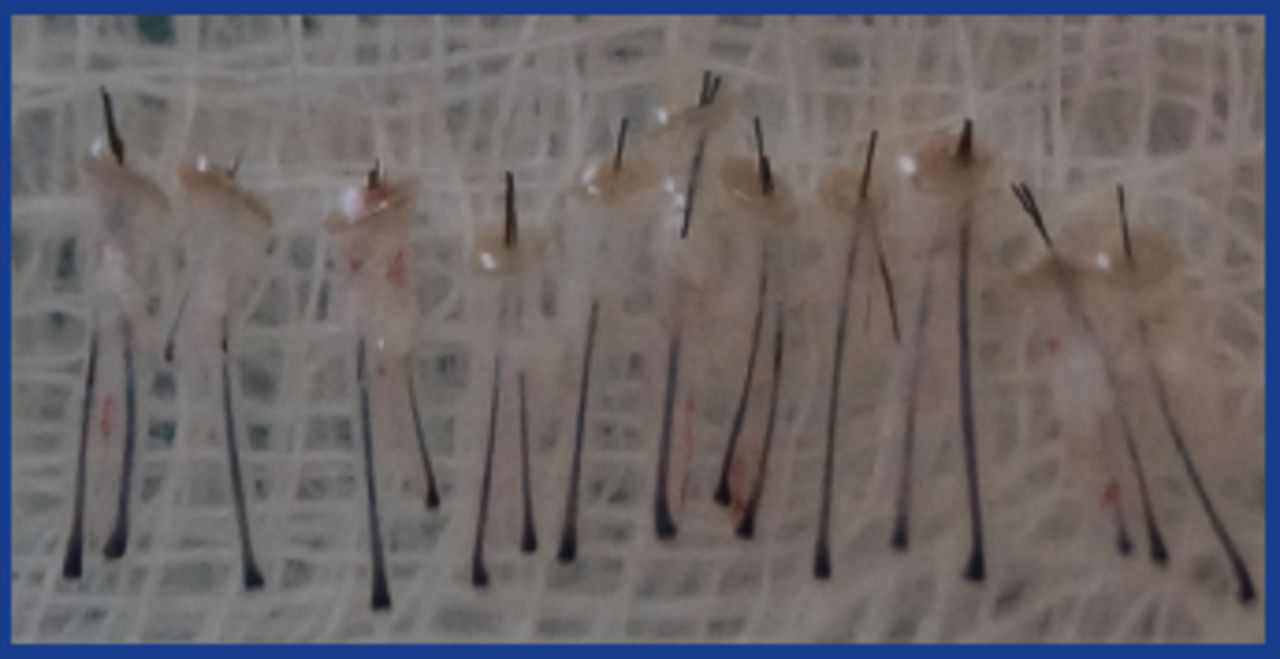
The density of the hair is less compared to the scalp. Kulachi reported in a sample of her patients beard density of 25-30 FU/cm2 and moustache density of 30-45 FU/cm2.5 These figures are probably low for many men. We found that the maximum density was over the chin and mid portion of the moustache. The caliber of the beard hair is more compared to that of the scalp (Figures 6 and 7). Beard hair is also typically more elliptical in shape compared to the circular or oval shape of scalp hair.
Beard graft

Scalp graft
Is the planning of a case of facial hair transplant different from that of scalp?
The basic principles of hair transplantation are the same but need to be planned in a different way. The physician needs to examine the whole face in detail when figuring out how many grafts will be required for every area of the beard and moustache that needs reconstruction. The most common patients that we encounter are the ones with congenital hypotrichia or atrichia. They often need as many as 2,500 grafts to re-create all of the beard and the moustache. Grafts are removed from the donor area in the same way as in a routine FUE. But the main difference is in the distribution of grafts and recipient site creation.
We can harvest with FUT for facial hair reconstruction but for lesser numbers of FUs most of our patients don’t want an invasive procedure with sutures and the resulting scar. Beard-to-beard is done if small scars are to be reconstructed requiring less than 100-150 grafts or for moustache reconstruction and the patient is willing to take grafts from the area under the chin. For the rest of the cases, scalp-to-beard is preferred.
Out of the seven zones of the beard, the sideburns and the cheek zone are the most important parts in the lateral profile. We prefer coronal slits because they help to ensure alignment of the hair acute to and parallel to the skin. Density is more in the upper part of the sideburn as the hair will grow in a downward direction and will provide better coverage inferiorly due to the overlapping effect of the hair from above. It is the same principle as we use to give a higher density in the part line of the scalp. The total number of grafts usually implanted in this area is around 200 per side.
When we reach the area of the cheek, the slits are directed in a skewed pattern as they turn laterally and downward. But this is quite a big zone and we further divide it into two parts, the border and the body. In the cheek border, we give less density and try to place the single-hair grafts to give it the look of the feathering zone.
The cheek body is where we give a higher density so that the maximum effect of a full beard can be achieved in this area. We usually place 2- and 3-hair grafts of scalp hair in this area. The density is less in the lowermost part of the cheek beard that merges with the jawline beard. There are 500-600 grafts required for the cheek beard on each side.
The jawline beard is again an area where a fullness effect is usually given by the hair layering from above, so a lesser number of grafts is required in that area. We usually do not implant any hair in the under area of the beard in the first sitting, as it is a shadow (or less cosmetically important) area and we want to implant a higher number of grafts in the more visible areas. The only exception is the alopecia caused by traction in the Sikhs, like the one shown in the image above, in which we need to reconstruct the undersurface of the beard (Figure 8).

Direction of hair in different beard areas: SB (sideburns)—downward direction; Ch (cheek beard)— lateral and downwards; JB (jawline beard)—down and laterally
The frontal aspect is cosmetically more important than the lateral aspect and requires a higher number of grafts compared to the lateral aspects. The total number of grafts for moustache and goatee reconstruction is usually around 1,000-1,100.
The moustache usually needs around 400-500 grafts. The density is higher (around 35-40 FU/cm2) and the hairs are directed downward. We tend to use sagittal slits in this area and make sure that the angle of the slit is as parallel to the skin as possible. We place a slightly higher number of grafts in the upper part as compared to the lower part of the moustache as the layering of the hair compensates for the lesser number of grafts in the bottom part. The single hair grafts are placed in the topmost row to give it a natural look.
The goatee is another area where a higher number of grafts is required (600-700). The main direction of the slits is inferior. In the upper part of the goatee, care must be taken not to apply too much force for making slits, as the skin is thin and the blade could penetrate the oral mucosa.
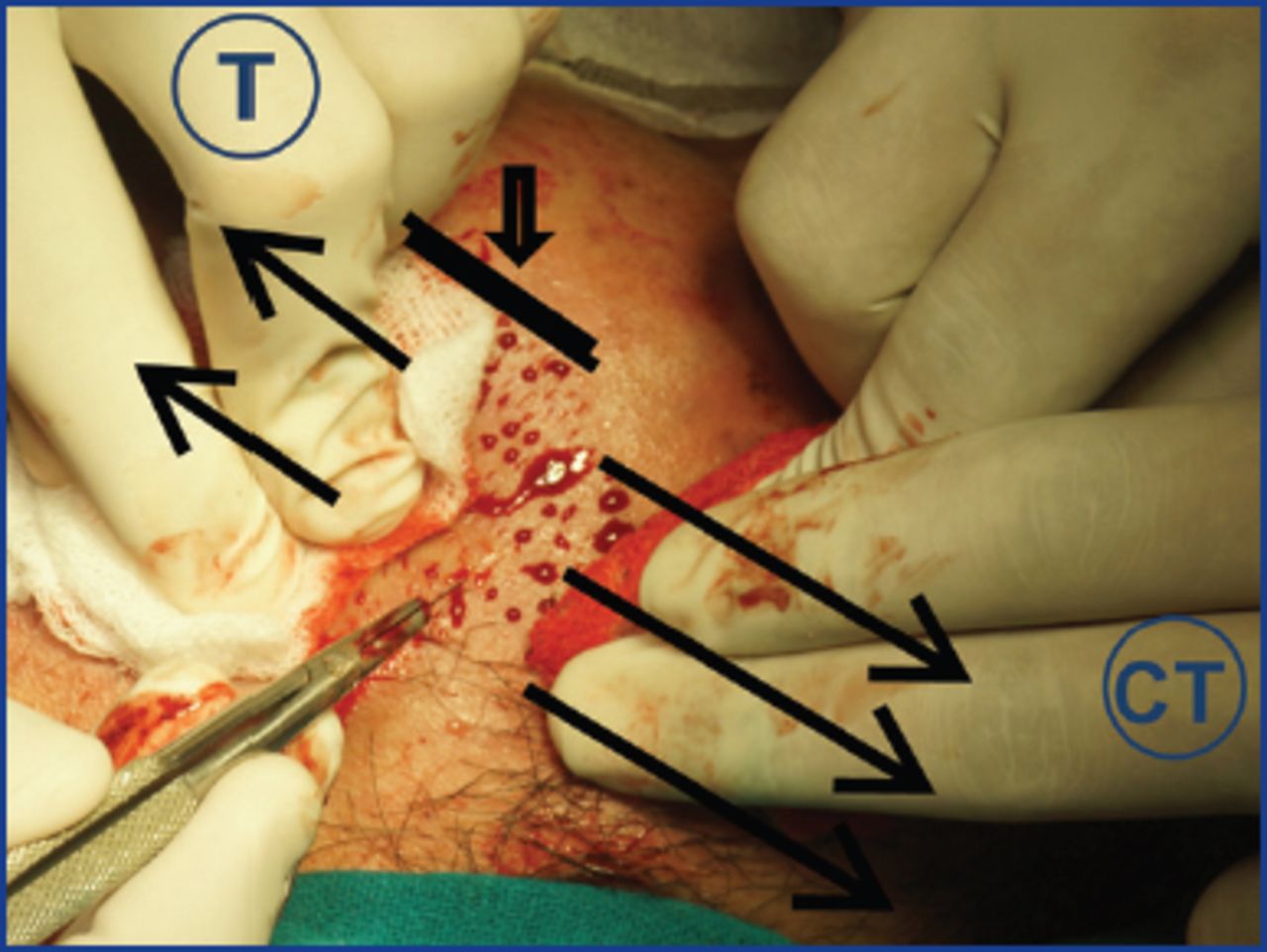
While making slits, adequate stretching and infiltration of saline is done to make the skin taut, as the facial skin is very loose. Thus, during creation of the recipient slits as well as during implantation, traction by surgeon and counter-traction by the assistant is done to stretch the lax facial tissue. Giving very superficial tumescence also helps to increase the turgidity and thus makes it easier during the procedure. At the time of implantation also, sometimes stretching is required to open the sites (Figure 9).
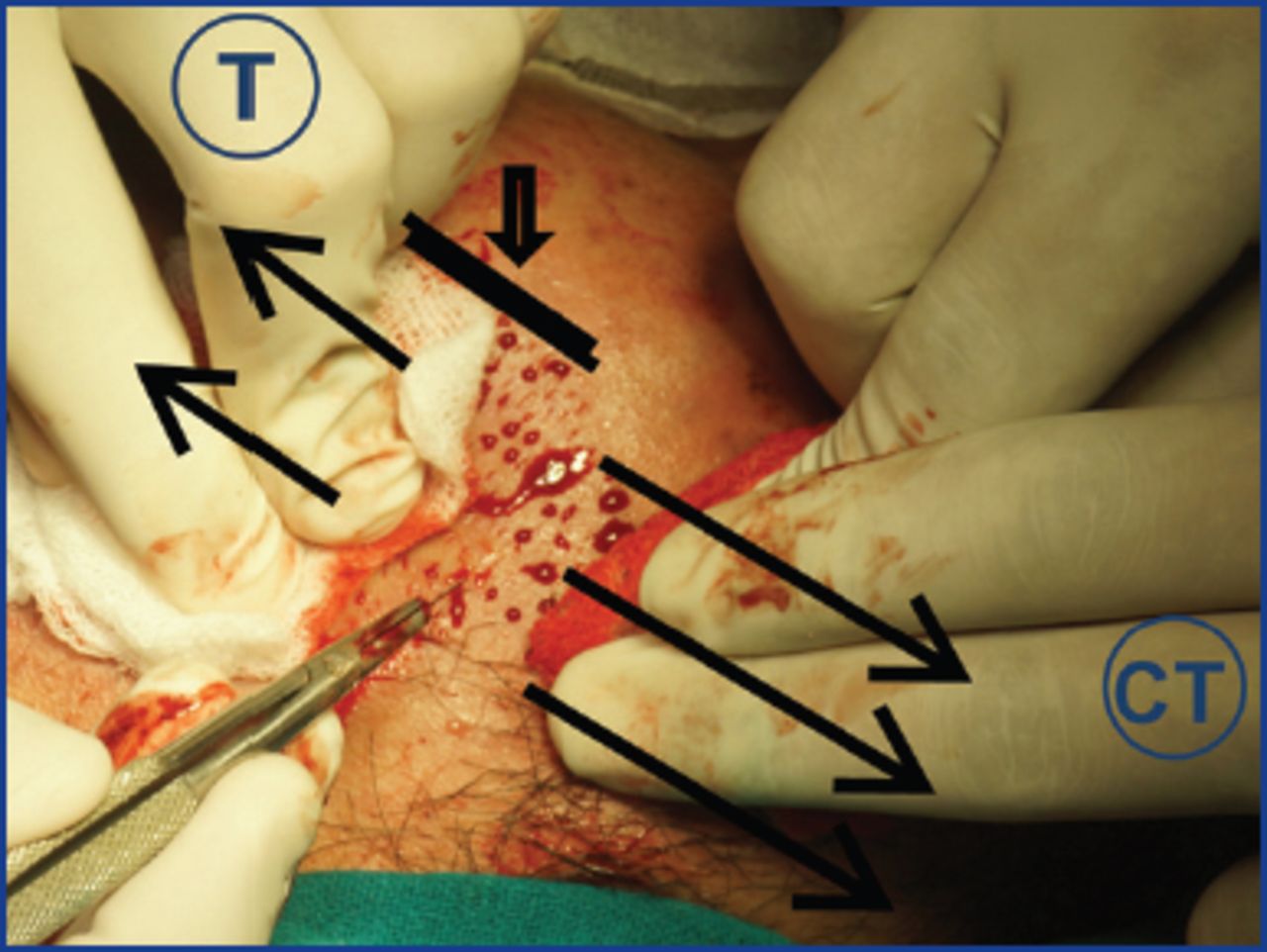
T (traction), CT (counter-traction). Note the direction and acute angle of the blade.
We usually make pre-made slits, but sometimes, the slits close before graft placement. When this happens, application of counter-traction to stretch the skin will reopen the sites for placement. Sometimes we use the stick-and-place method in which this problem of site closure does not happen.
Donor Area
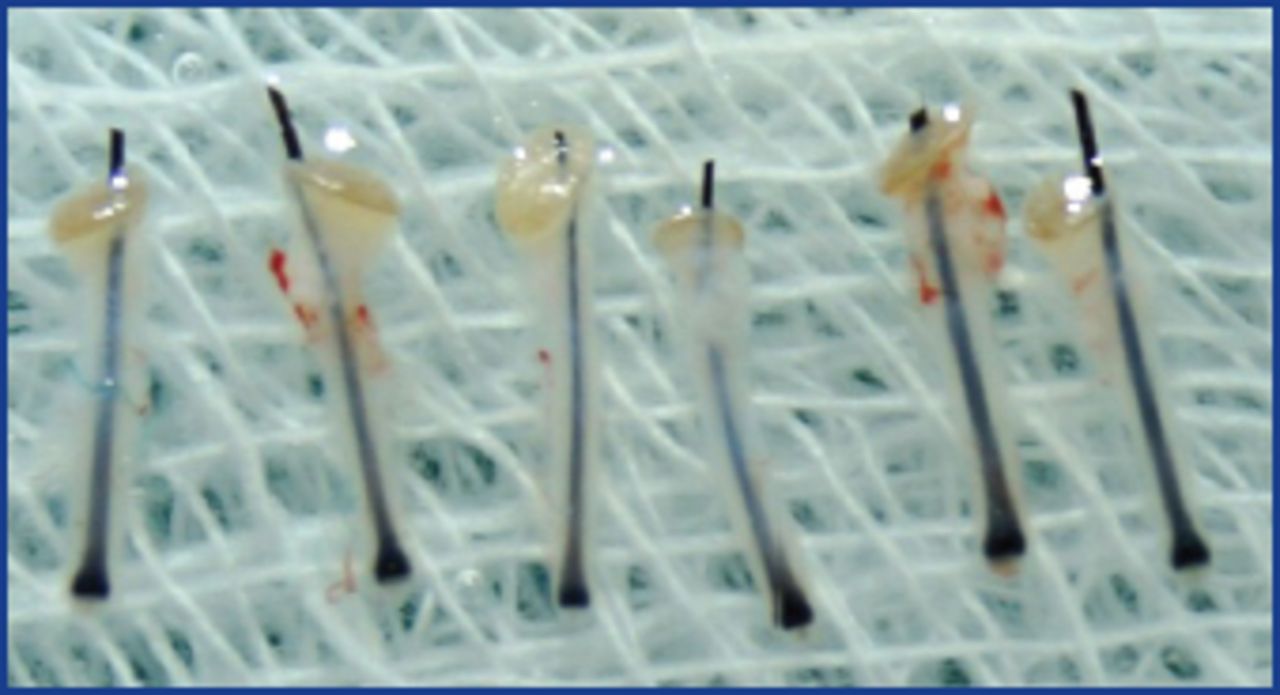
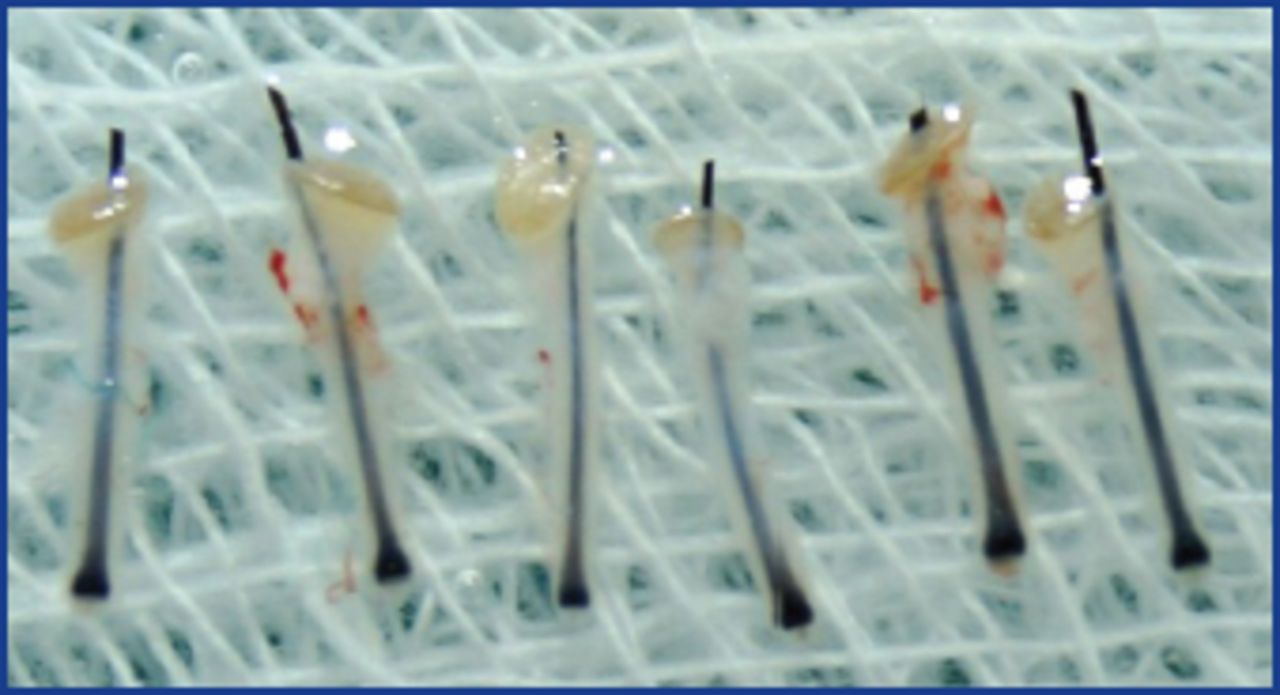
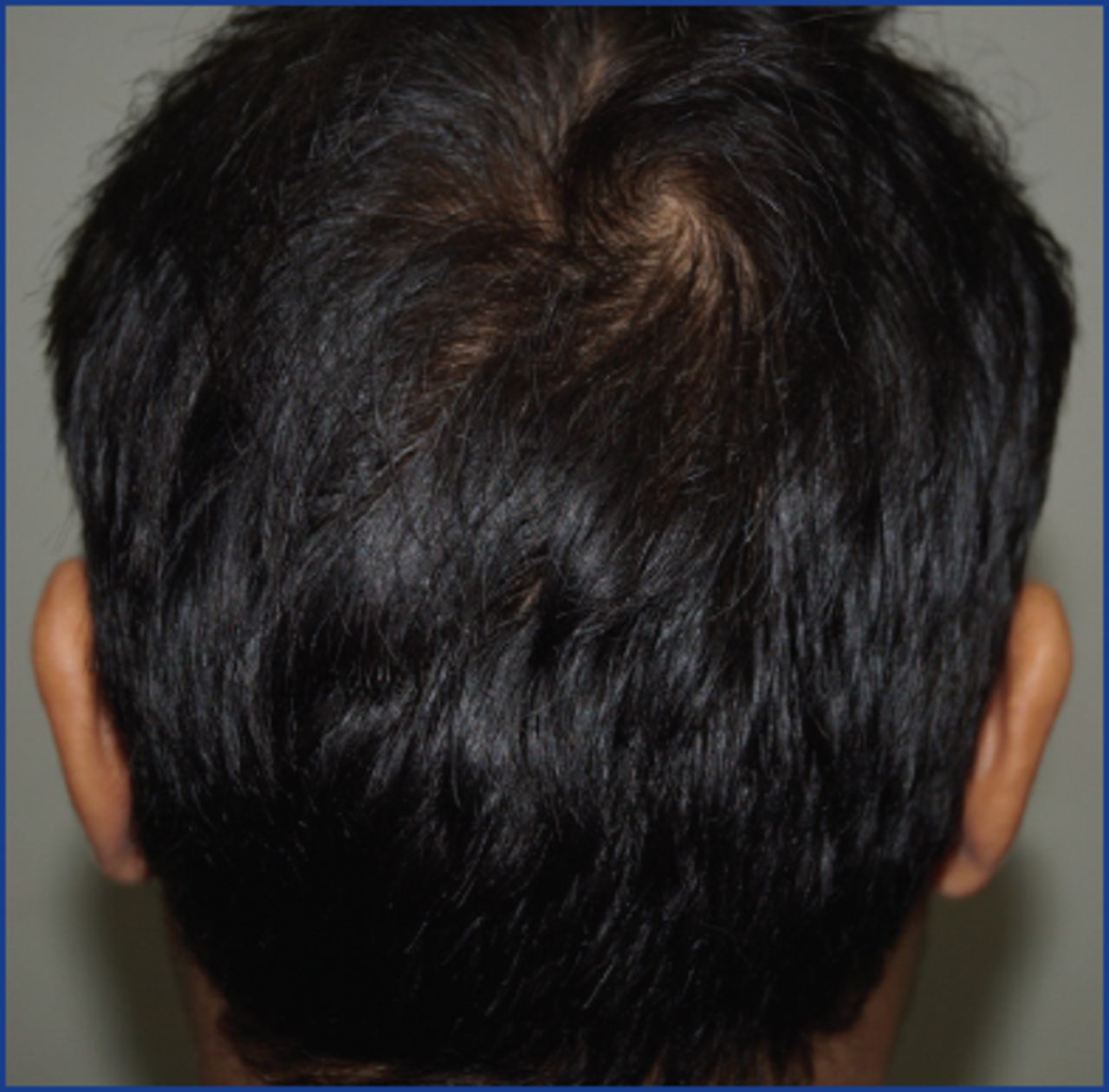
We prefer scalp as the donor area for beard, and scalp as well as beard if moustache or small areas of beard are reconstructed. We take out the grafts from the mid-occipital area by FUE and mostly 1- or 2-hair grafts are extracted (Figures 10 and 11).
Donor scalp; mid-occipital area is preferred.

Donor scalp trichogram; 1- and 2-hair grafts preferred
Precautions During Implantation
During implantation, 1-hair grafts are placed over the superior outline similar to scalp hairline, and 1- or 2-hair grafts over the other areas. Two-hair or paired grafts can be used to increase the thickness. Implantation takes a longer time compared to scalp (Figure 12).

Upper zone for single hair grafts only
What is the technique of giving local anesthesia in the recipient areas?
Local Anesthesia
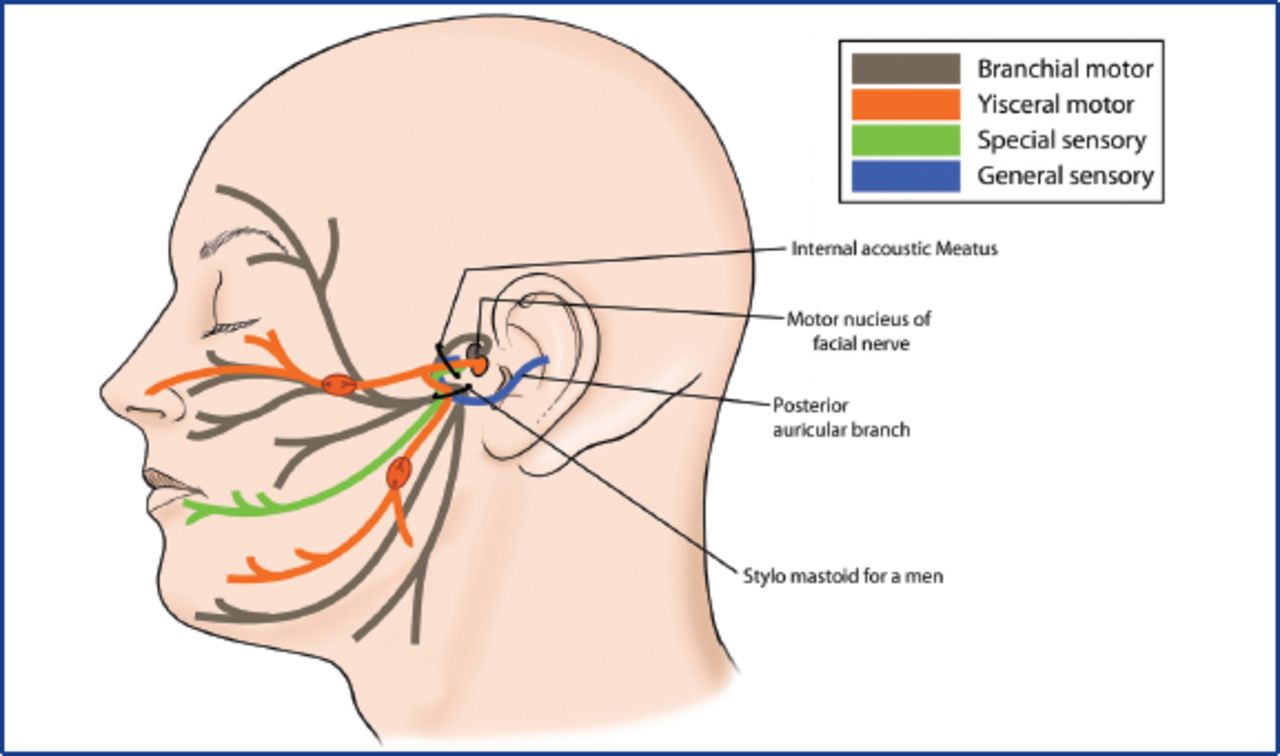
Local anesthesia is very painful in the facial area (Figure 13). Therefore, we have started giving nerve blocks. The blocks that we give are as follows:
Auriculotemporal nerve: This is blocked as it ascends in front of the auricle over the posterior root of zygoma, behind the superficial temporal artery. The needle is inserted about 1.5cm anterior to the ear, at the level of tragus behind the superficial temporal artery pulsations and around 1ml of 2% Lidocaine with 1:200,000 Adrenaline is injected.6 This nerve supplies the skin over the parotid gland, the external ear.
Infraorbital nerve: This is blocked by giving 1ml of the 2% Lidocaine with 1:200,000 Adrenaline through the intraoral route by inserting the needle vertically upwards with tip pointing towards the foramen in the gingivolabial sulcus between the canine and the first premolar. This anesthetizes the infraorbital area, upper lip, and moustache area.
Mental nerve: The nerve is blocked as it emerges from the mental foramen, which is located at the gingivolabial sulcus between the two lower premolars (1ml of 2% Lignocaine with 1:200,000 Adrenaline) This helps to numb the lower lip and chin area.
Long buccal nerve: This is blocked by injecting 2-3cm lateral and superior to the angle of the mouth with needle pointing towards mouth and in a fanning manner. This nerve supplies the cheek area.7
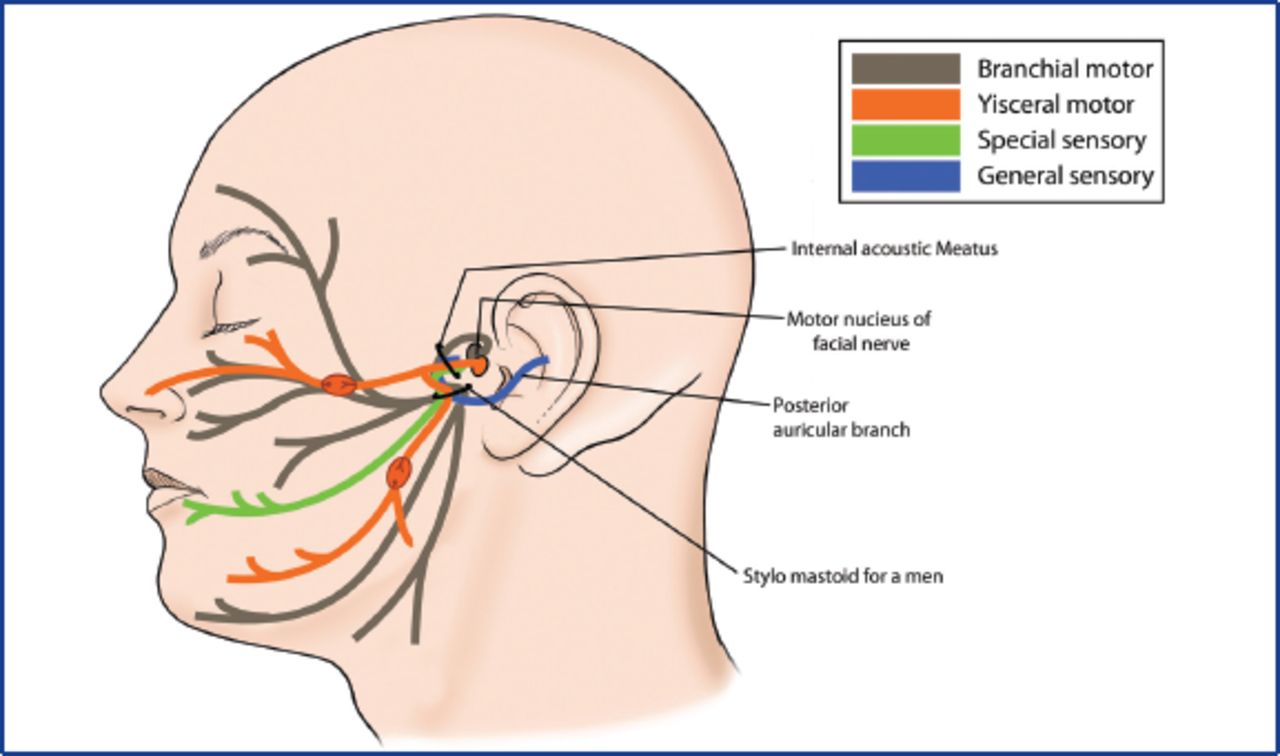
Nerve supply of the face
After the nerve blocks, field anaesthesia is given starting from in front of the ear advancing downward to the lower border of the beard, then across the lower border and then over the upper border (Figure 14).

Giving local anesthesia to the beard area
Post-operative Precautions
During the post-operative period, some drooling may occur on the first day due to the local anesthesia, so we advise semisolids on the day of surgery after discharge. Hair growth begins around 3 months and improves over the next year. Superficial tumescence can also cause post-op ecchymosis, which disappears over a couple of days.
Results after Facial HT
Results from facial transplantation are shown in Figures 15-19.

Patient 1, before (left) and immediate post-op (right)

Before (left) and after 1 week (right)

Patient 2, before (left) and after 6 months (right)

Patient 3, before (left) and (100grafts) after 1 year (right)

Patient 4, before surgery (A); immediate post-op (B); and after 2 years (C)
- Copyright © 2015 by The International Society of Hair Restoration Surgery
In this issue









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.