

Abstract
In my recent travels, I have seen the best hair transplant results in my 38 years of hair transplant experience. From a technique that many consider obsolete! Drs. Damkerng Pathomvanich and Jerry Wong present their FUT expertise and results as the lead article for this edition. Comments from other experts, for and against FUT, follow. I’m looking forward to seeing equally impressive FUE results. —MM
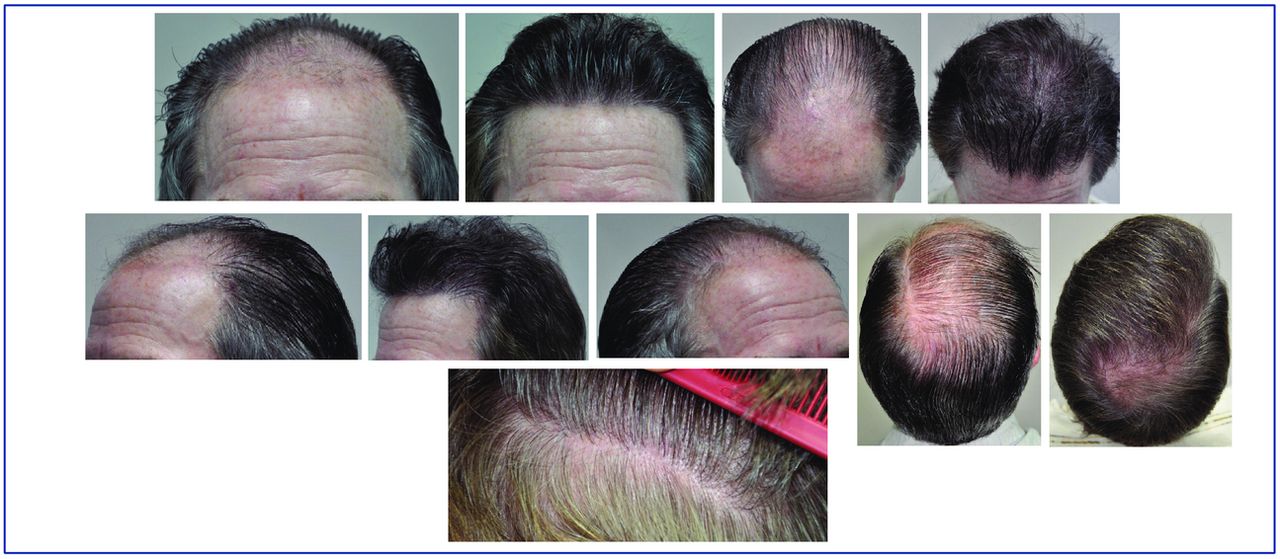
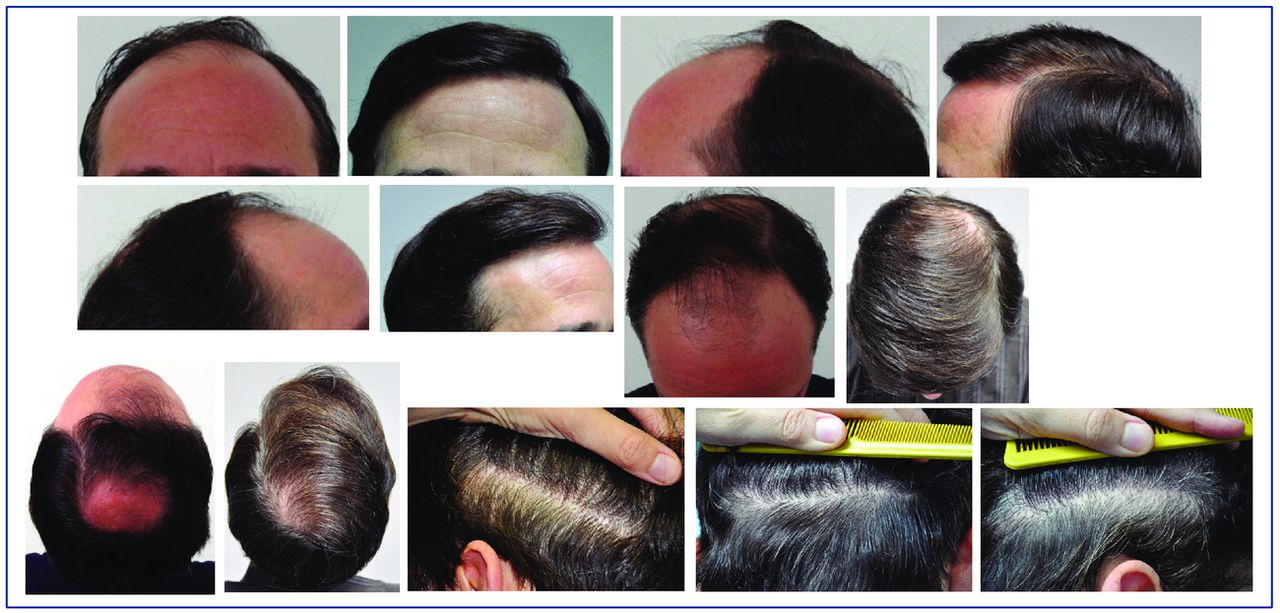
In reality, the patient comes to see the doctor just to have his hair loss restored to achieve a result that is as dense as possible, as natural as possible, and, of course, in one go. FUT has stood the test of time with good results and minimal donor scaring in the majority of cases. See the before and after photos in Figure 1. However, the technique of donor harvesting today has swung to what is advertised as scarless and painless surgery of follicular unit extraction (FUE) either by manual, power punch, or robot. I believe that no scar means no hair is extracted! There has to be scarring of some nature.

Before and 10 months after hair transplant (FUT); 3,066 grafts (6,732 hairs) with minimal donor scar.
With experience, some FUE surgeons are now able to extract large quantity of grafts, some exceeding 3,000 to match FUT numbers. However, we need to see more good results with good growth and need to see less diffuse thinning from over harvesting the donor area. To me, diffuse thinning after excessive FUE is far worse than a strip scar, since the diffuse thinning from FUE looks like a disease of the scalp and cannot be well camouflaged. The FUT linear scar, even a wide one, still can be hidden by the hair bangs above the scar.
In my opinion, in FUT we use all the hair in the entire strip that is harvested. The grafts that are microscopically dissected contain all supporting tissues whether they are vital to hair growth or not, but it certainly helps to prevent desiccation and trauma during insertion. The grafts taken via FUT can be dissected into any size graft that the surgeon needs (e.g., 1-2 follicle unit grafts). The graft loss from the entire process of harvesting and cutting with open technique and high magnification loupe should be 1% more or less; my last report 15 years ago was 1.98% without using magnification.1 My curiosity is how the blind technique with FUE reported a very low transection rate at 2-3% (I’m sure this would have been checked under microscopy), in good hands of course. However, there can be trauma to the grafts during extraction by using forceps, and the extracted grafts are naked, which may be a concern during graft insertion and then their survival. FUT reports on graft survival are at about 90%.2 Is the FUE growth rate getting close to FUT?
FUT harvesting can ensure that all hair grafts are taken at the permanent zone. With appropriate checking of scalp laxity by Mayer,3 Laser lax device,4 and Rassman’s Laxometer,3 the surgeon is able to excise a strip of appropriate width with more confidence. The surgeon should be careful and skillful to minimize transection during harvesting and to avoid hematoma and dessication. If the wound is approximated with minimal tension using trichophytic closure and proper alignment of the hair direction, the scar will be very small at 1-2mm 90% of the time. In FUE harvesting, on the other hand, if the grafts are extracted either too high or too low, they are not in the safe zone and future graft loss will be experienced in the recipient area and the small round donor scars may be exposed.
In most offices, the cost of FUT to the patient is lower than FUE even though more grafts are involved. With time, this is changing, and in some offices the prices are the same.
FUT harvesting and graft dissection are a team effort. FUE is only done by a single surgeon, thus causing overall fatigue, eye strain, tennis elbow, carpal tunnel syndrome, and myofascial pain to the hair surgeon. It is less delegatable than FUT.
Subsequent sessions either by FUT or FUE are a challenge and difficult, both result in more scar and more transection than the virgin scalp. FUT might result in wider scar if the same scar is used and FUE will end up with diffuse thinning at donor area.
With the advance in micro-pigmentation expertise, the scars from FUE and from FUT can be camouflaged if performed well by experienced operators. This is a very welcome addition to our patient help armamentarium.
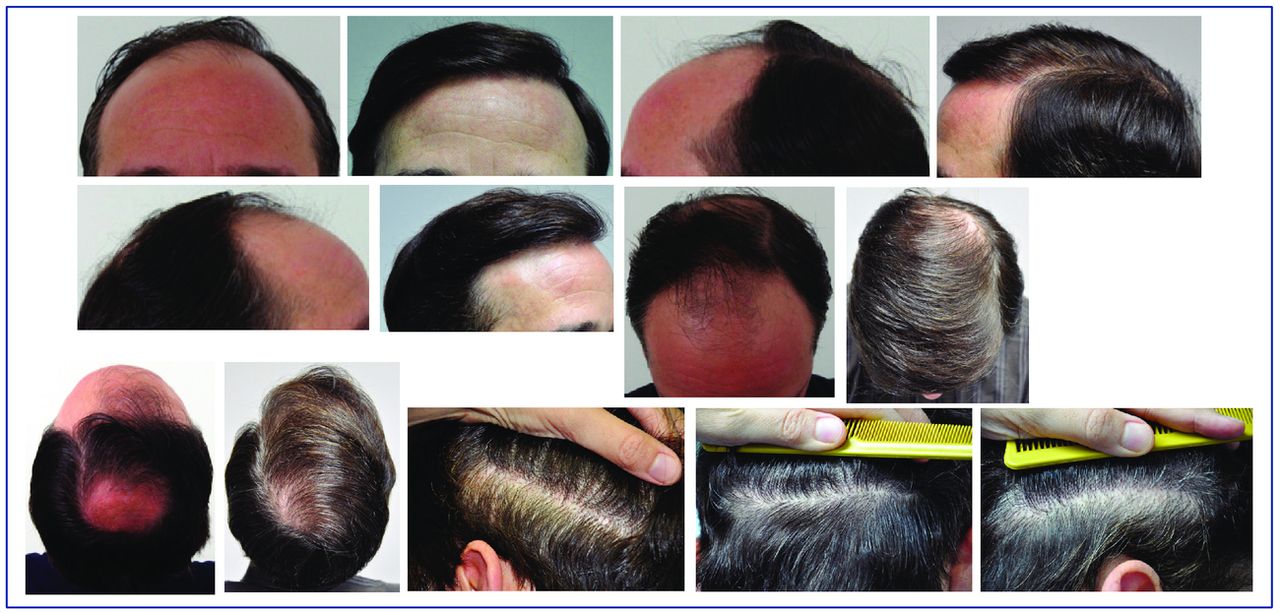
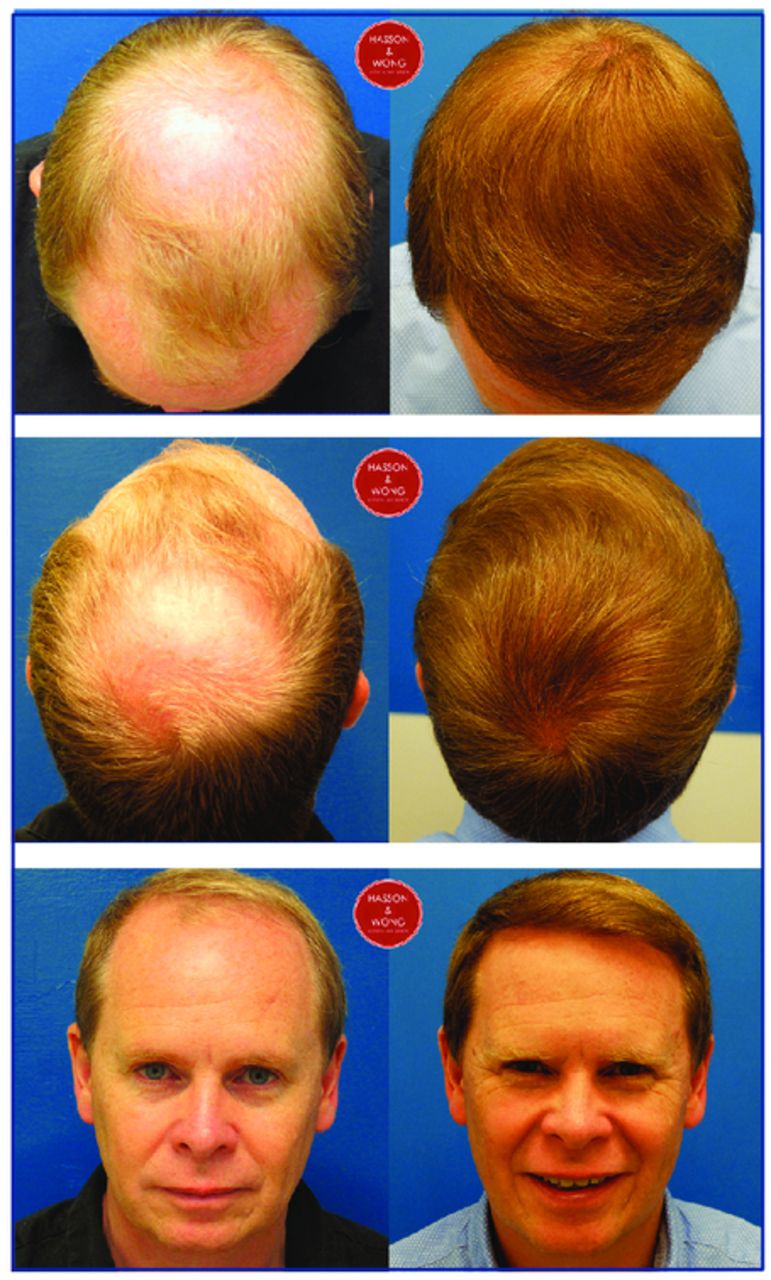
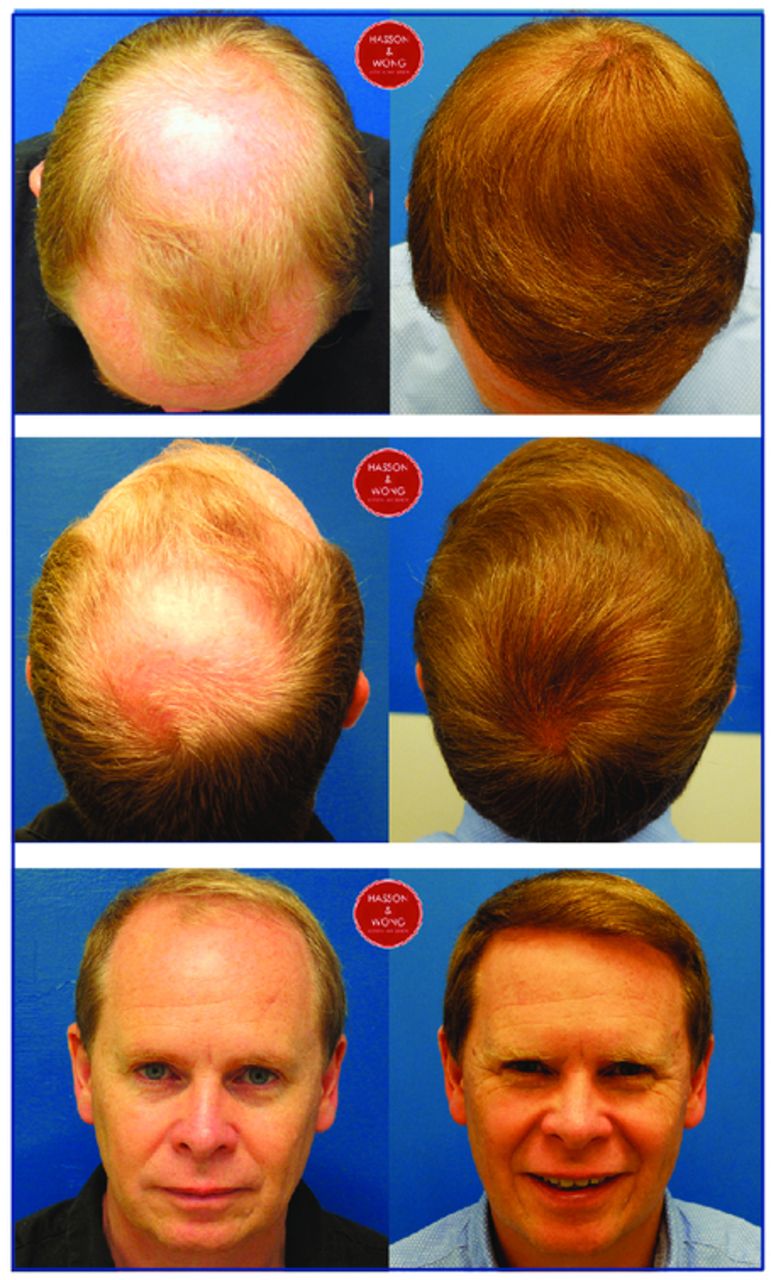
Lastly, it is not only the scar from either FUE or FUT that is important for the patient, but the result of the transplantation that concerns them most. Until we see a lot of cases of excellent growth from FUE that can match the well-established FUT, for me, FUT wins hands down. (See the photos in Figures 2 and 3 for before and after photos.)
Before and after hair transplant (FUT): 3,864 grafts (8,971 hairs) in one session with minimal donor scar.
Before and after hair transplant (FUT): 5,692 grafts (11,256 hairs) in 2 sessions with minimal donor scar
The 3rd Mediterranean FUE conference has just completed and what I saw was certainly an eye-opener. Having watched what I believe to be some of the best in the world in action has given me a whole new understanding of FUE. FUE, if it is performed well as demonstrated by Drs. Lorenzo, Erdogan, Devroye, and Cole, can and does generate excellent results.
After seeing just how labor intensive and time consuming FUE is, I also have a whole new appreciation of FUT and having a well-trained team that can generate 5,000 perfectly trimmed grafts in just a few hours. I feel absolutely spoiled that I have the luxury of so many grafts to use in a single surgery. Over the years, we have encouraged each team member to try to aim for zero wastage. Impossible to do, but it does give each team member a target to aim for and now we rarely see any transected hairs from the dissection process. I believe the single most effective way to remove donor hair in large quantities is with the strip.
One of the best strip techniques of minimizing hair lost is Dr. Pathomvanich’s open technique. This technique of scoring the surface and skin hook dissection is so adaptable that it can remove hair successfully even in the most difficult cases. Hair with extreme curls, hair with excessive splay, hair misdirected and imbedded in scar tissue can all be extracted with minimal waste. This method has a prolonged learning curve and adds an extra 30-40 minutes to the strip removal. Adopting this technique has made me a better surgeon in that I now know I can remove hair under any condition without fear of transection. When the team sees the extra effort the surgeon makes to preserve hair, it sets the tone for the surgery.
Most Norwood VI patients will be happy with the growth from 5,000-7,000 FUs. Some will want coverage that only 10,000-plus grafts will provide. It is vital that we do the detailed work as a team to minimize wastage so that we can provide the extra coverage for those patients that want more.
For most clinics doing mega sessions, strip surgery is the workhorse that day in and day out handles the majority of the large sessions. A lot of clinics now have the experience to do mega strip sessions with consistently good results. Strip mega sessions are time efficient in that 5,000-plus grafts can be routinely done in one day and the patient may not need another surgery for a long time. If more coverage is desired, a second procedure is usually all that is required. In patients with good laxity and density, even after 10,000 FUs have been removed the linear scar that remains is very thin and easily concealed by hair. The majority of the donor area is essentially pristine and untouched. Should the patient ever desire to shave his head, the scar can then be revised if needed and softened with FUE.
There are a handful of talented FUE surgeons that can do 5,000-plus grafts providing excellent growth and coverage while leaving the donor intact with minimal scarring. They are but a handful. Top-notch strip surgery is difficult, top-notch FUE surgery is even more difficult. Both surgeries, if performed by the inexperienced and the unskilled, can be very damaging. A bad strip surgery will leave a big scar, poor growth, etc. Most patients will recognize this as bad work and seek another surgeon for repair work. In these cases, there is usually sufficient donor hair left for the repair. There are many FUE clinics offering mega FUE sessions that do not have the expertise nor the experience to do such work. They can effectively wipe out the entire donor area with “one” FUE mega session by extracting over several days.
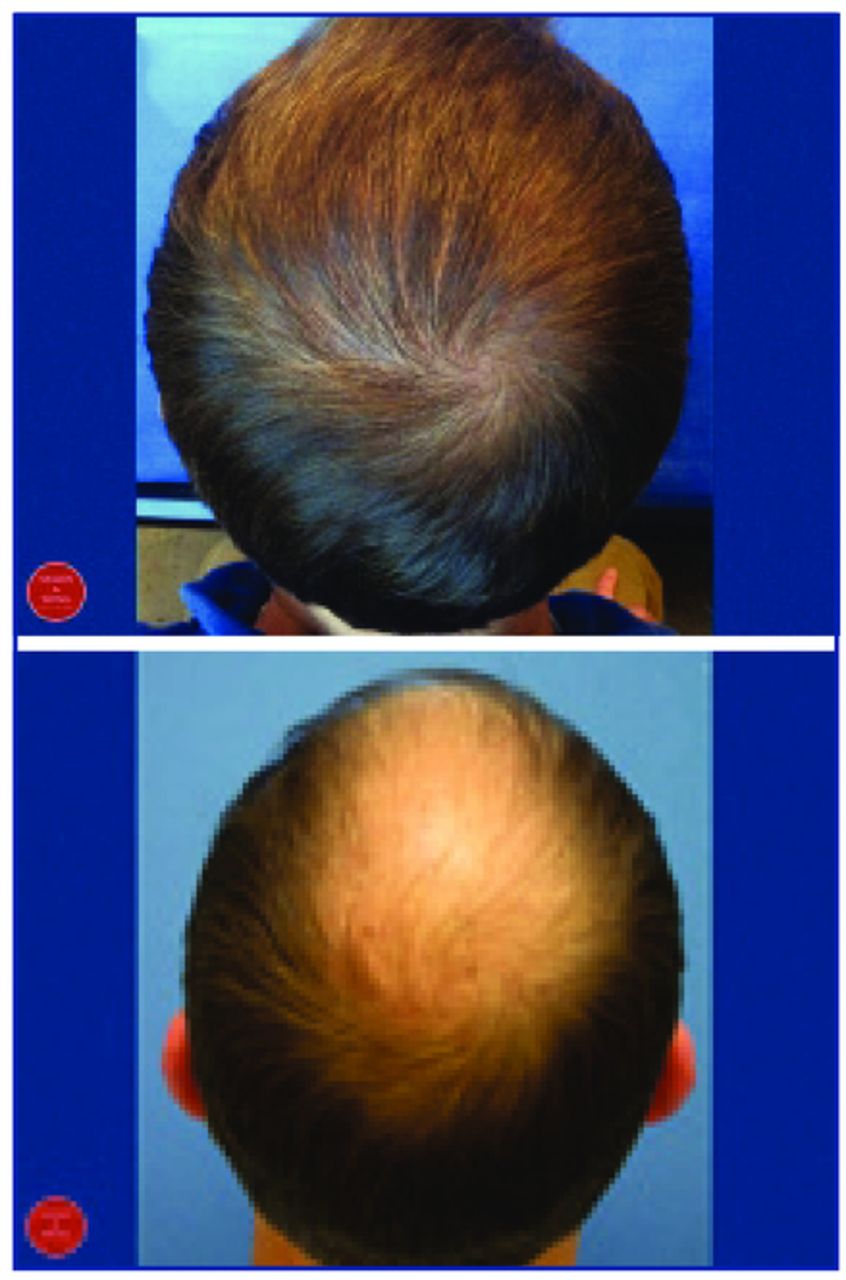
Right now, strip has the edge over FUE in terms of total numbers of grafts that can be removed and the consistency of the overall growth rate. The two patients shown in Figures 4 and 5 have had two surgeries each with grafts totaling 8,000-10,000. Both have small linear scars and intact donor with more hair in reserve.
Before and after hair transplant (FUT): 7,111 grafts over 2 surgeries.
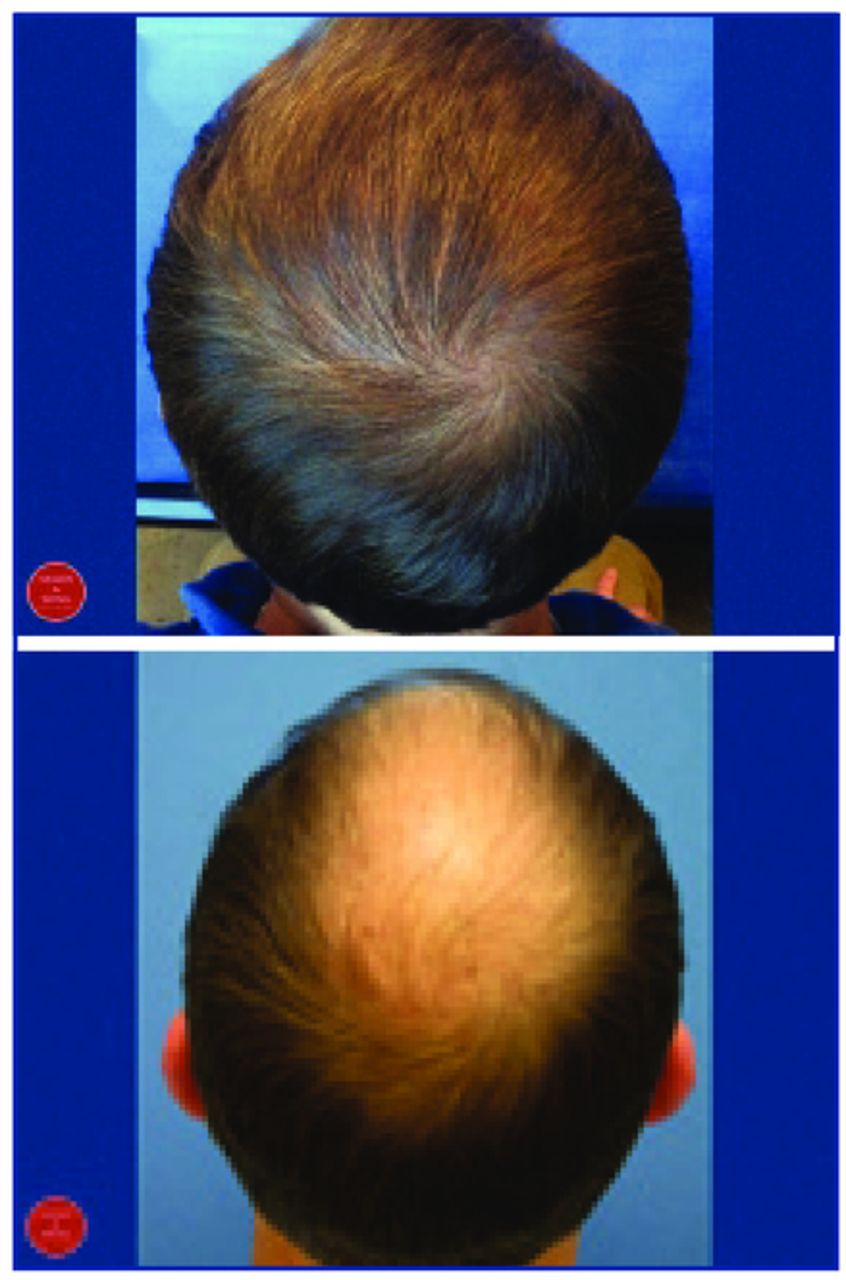
Before and after hair transplant (FUT): 9,100 grafts over 2 surgeries.
Physicians Sound Off: FUT vs. FUE
Mike Beehner, MD, FISHRS
I firmly believe that choosing strip harvesting with microscopic dissection over FUE as the principal means of obtaining donor hair is a “no-brainer.” The reasons are many:
The donor strip is taken from the mid-level hair, which will be least affected by the progression of male pattern balding. This is not true with FUE, which often harvests from a large area that includes the upper fringe and lower nape area.
FUT grafts are carefully dissected under a microscope with high magnification to ensure that perfect grafts are obtained, versus the “plucking” involved with FUE, which in a high percentage of grafts results in much of the surrounding fatty tissue being torn off, leaving a naked lower follicle.
FUT is more easily learned by the average cosmetic practitioner, whereas FUE is a difficult task to master and often results in inconsistent or poor graft survival.
An MFU graft can be dissected from a strip, whereas this is impossible with FUE.
The overall “scarring” effect from FUE, in my opinion, is far more than that obtained by a strip through the central height of the donor tissue.
Strip FU grafts are easier for the placers to safely insert into recipient sites without damaging the grafts, thus ensuring high survival.
Robert M. Bernstein, MD
FUT should neither be considered the preferred hair restoration technique nor be deemed obsolete and abandoned. Both FUT and FUE are excellent techniques, but they have different clinical indications. In my opinion, to deliver the best care for our patients, hair restoration physicians should have expertise in both procedures, and they should offer both in their practices.
The main advantage of FUT is that it typically (but not always) gives the highest yield of hair. Therefore, when the patient’s primary goal is to achieve maximum fullness, FUT should be performed. There are many well-described reasons for this, including the precision of stereomicroscopic dissection and the ability to efficiently harvest from a more select area of the donor zone, but these are beyond the scope of this brief commentary.
The main advantage of FUE is no linear scar. Therefore, when the patient’s primary goal is to be able to wear his hair very short, FUE should be performed. FUE is also indicated when there is an increased risk of a widened scar or when scalp laxity does not permit a strip excision. The patient may sometimes choose FUE simply to avoid the stigma of a linear donor scar.
There are situations in which both procedures are useful in the same patient. For example, FUT may first be used to maximize yield, but then, after several sessions, the scalp may become too tight to continue to perform FUT, or the donor scar may become wider than anticipated. In the former case, the physician can switch to FUE to obtain additional grafts; in the latter case, FUE may be used to camouflage the scar of the FUT procedure.
It is tempting to see the world in black and white, and it is easiest to learn and train one’s staff in just one hair transplant technique—but medicine is never so simple. Developments over the past 20 years have given us two excellent hair restoration procedures. We should offer our patients both.
John P. Cole, MD
In any field of medicine where hand-eye coordination along with attention to detail is required, there are physicians who consistently achieve superior results. One cannot debate the merits of strip surgery versus FUE based on results alone. Furthermore, false advertising is not limited to FUE, where some physicians claim it is scarless. Many proclaim that FUT leaves a paper-thin scar, which most certainly is not always the case.
What we must do is break down the benefits of both procedures in a comparison and address the perpetual false misconceptions of FUT proponents. —John P. Cole
What we must do is break down the benefits of both procedures in a comparison and address the perpetual false misconceptions of FUT proponents. I am in a particularly rare position to argue the benefits of both since I have performed over 8,000 FUT procedures and nearly 6,000 FUE procedures. There are some benefits to FUT. FUT is far less laborious to the physician. The physician can perform more grafts in a single day with less effort primarily because surgery time on any case is less so the physician can perform large surgeries on more patients. With a skilled, well-managed team, it is easier to obtain a low follicle transection rate with FUT. In some instances, donor scarring from a large FUT procedure is much less noticeable than from many FUE procedures.
Why did my practice swing from FUT to FUE after more than a decade focused on reaching perfection with FUT? Let’s first consider how the world looked in 2002 when I began earnestly exploring FUE. Only one clinic in the world offered FUE and they refused to show their technique to anyone. No one else in the world had a technique to produce consistent results or knowledge of how to manage the donor area. We were the blind leading the blind. If no one knew how to perform the procedure well, how did FUE initially take root? Many patients wanted the procedure because it was less invasive and many patients hate strip scars. Because these patients wanted to avoid strip surgery, they were willing to allow physicians such as myself to develop tools and techniques to produce consistent FUE results. FUE rapidly became the procedure of choice by patients.
Over time, we were able to reduce the follicle transection rate with manual dissection to fewer than 3% with sharper punches along with variation in punch size and depth of incision. With mechanical dissection, the follicle transection rate can be higher, so it is advisable for the surgeon to know both manual and mechanical FUE. As with any delicate surgical procedure, small alterations in technique produce significant improvements in results. In FUT, assistants in most practices dissect all of the grafts. When assistants dissect the grafts, the physician has limited control over quality. In FUE, the physician has total control over the dissection of the grafts.
When a follicle is transected during the graft dissection process of FUT, the assistant generally discards it. In FUE, transected follicles remain in the donor area where they have the potential to survive the bisection.
We must recognize that hair loss is a perpetual process that worsens over time. Patients will want a second or third or fourth procedure as their hair loss progresses. Strip scars are often thinner after a single FUT. It is these subsequent procedures that commonly produce wide scars. Any time you perform a strip procedure, you alter hair growth angles. The disruption of the natural geometry of the donor area worsens with subsequent surgeries. Eventually, hair on the inferior margin of the scar elevates producing the dreaded horse’s tail. Furthermore, the width of a strip scar is unpredictable even after a single procedure. Finally, patients often deplore their strip scar even when it is 1-2mm wide.
In any patient, the total number of follicular units is the same. It is ridiculous to suggest that over time you can magically produce more grafts through FUT. My cross-sectional trichometry (CST) studies show that the CST decreases more following FUT than FUE. The marked decrease in the CST from strip surgery is secondary to a loss of follicles most likely due to traction alopecia. The CST is maintained from FUE because the donor area contracts approximately 12% resulting in maintenance of the follicular unit density. In FUT, the remaining skin must cover the void created from the strip removal. Stretching the skin to cover this space results in a decrease in follicular unit density, particularly adjacent to the scar. Follicular unit density necessarily decreases when fewer follicular units must cover the same surface area.
As strip harvesting progresses, the CST decreases further, angle distortion increases, and scars widen. Those with maximal hair loss often thin in their donor area as well, since the donor area in these individuals is not permanent. Patients in their 50s often find it difficult to conceal their strip scars, especially when their hair is wet. It stands to reason that those with maximal hair loss need the most number of grafts. This often exposes scars. Thus, the potential to harvest from the donor area either from FUE or FUT screeches to a halt.
Rather than a lower capacity to obtain grafts from FUE, FUE offers a larger supply because hair must not be left in the donor area to conceal the scar. In FUE, the physician has the capacity to harvest outside the traditional “safer” donor area because only 3% of men will advance to a Norwood VII by age 60. This leaves an abundant supply on the sides of the head. Furthermore, the physician may often harvest from the more inferior portion of the donor area with FUE where strip harvesting typically produces the widest scars regardless of technique or physician skill.
The overall management of the donor area is different with FUE than with FUT. If the physician harvests only from the traditional “safer” donor area alone, the donor area appears thin in the harvested area and thick in the surrounding areas. In those with maximal hair loss, the goal from FUE is to produce a similar density throughout the donor area and the recipient area primarily by harvesting from all over the donor area. Furthermore, taking portions of the follicular group with smaller punches produces minimal scarring and hypopigmentation because color is maintained better due to circulation to the remaining follicles in the follicular group along with pigmentation from the remaining hair follicles. If hypopigmentation does occur, scalp micropigmentation (SMP) to the hypopigmented areas produces the appearance of a normal scalp even with the head shaved. The result from SMP is far superior with FUE than with FUT. It is nearly impossible to resolve hair angle distortion from FUT, especially when a horse’s tail forms.
Large numbers of grafts are often produced from FUT resulting in more than 5,000 grafts in some instances. This number is generally obtained by splitting the follicular groups and follicular units by the assistants. This can be termed “sub-follicular unit” transplantation. In FUE, we may choose to take pieces of the follicular unit or group with smaller punches, as well. A physician could do this with the entire 15,300 follicular groups that exist in the average Caucasian donor area with FUE.
In summary, FUE is by far the preferred procedure with patients. The entire dissection is under the control of the physician. FUE may produce a higher transection rate, but the transected follicles remain in the donor area. Subsequent procedures do not produce the undesirable effects that subsequent strips produce. FUE maintains the donor area CST better than FUT. Donor area thinning from FUE may be managed by harvesting outside the traditional “safer” donor area giving patients a greater supply of hair follicles when they are young and a full crop of hair is more important to them. SMP may be used to manage hypopigmentation leaving the appearance of a pristine donor area. Most importantly, skilled hands produce the same results and yields for both FUE and FUT surgeons.
Bob Haber, MD, FISHRS
The Safe Zone. Really only those three words are needed to expose the greatest problem of FUE. We have recognized for many years that as hair loss progresses, the safe zone, well described by Dr. Walter Unger in his many texts, remains essentially unchanged. And while most men will not progress to a Norwood Class VII, many of the young men undergoing aggressive FUE will indeed progress that far. FUT surgeons harvest 100% of their grafts from within the safe zone, and can easily obtain 6,000 or more grafts from that area. In contrast, EVERY surgeon performing FUE must harvest far above and far below this zone in order to obtain a comparable quantity of grafts, and must leave behind thousands of the most ideal transplantable grafts in order to provide coverage for the donor area. What will happen as many of these men progress in their hair loss? The hairs harvested from the risky areas outside the safe zone will be lost, the small FUE scars will become visible, and a new generation of unhappy hair transplant patients will be born. Equally troubling about FUE is transection. While an elite group of master FUE surgeons can harvest with a low transection rate, the vast majority of FUE surgeons damage easily 20% of all the hairs harvested. The true magnitude of these lost hairs may never be known to the patients, but our Hippocratic oath demands that we place the best interests of our patients above all else.
The Safe Zone. Really only those words are needed to expose the greatest problem of FUE. —Bob Haber
Carlos Puig, DO, FISHRS
New technologies in hair restoration surgery are slow to be totally understood, probably because it takes so long to see the final result of your surgery. New technologies must provide high-quality results that are reproducible by all physicians. Historically speaking, the timeline for demonstrating safety and reproducibility appears to be about 8-10 years. It was that way for FUT vs. the plug, the scalp reduction, and Juri and Frechet flaps. We are on the cusp of that timeline for FUE, and are just now beginning to have enough multi-center experience with the procedure to notice its flaws and limitations.
What ultimately endures are the techniques best suited to provide the optimum results for patient care, not the technique that most satisfies the physician’s ego. —James Vogel
Drs. Paul Rose, John Cole and I noticed a few years ago that we were seeing more FUE cases with what appeared to be overharvested donor areas, the “moth-eaten” see through look when the hair was worn longer, at 2 or 3cm. This is never noticeable if the patient wears their hair real short. I have come to realize that this appearance is not, as suspected, the result of overharvesting, but rather a result of the fact that FUE procedures lack the biological creep routinely seen with FUT donor harvesting.
Because FUT wounds are closed with mild wound tension, there is some biological creep that occurs in conjunction with the redistribution of donor hair above and below the wound. This biological creep produces normal skin between the remaining hairs in the donor area. The FUE procedure produces no wound tension, and hence no biological creep. The area between the remaining donor hair in an FUE harvest is replaced with scar, which reflects light more than normal skin, producing this moth eaten appearance when the hair is worn long. The important question is at what total graft count of FUE harvesting does this phenomena begin to limit the patient’s ability to grow his or her hair long?
I believe an honest critical eye will see this donor area sparseness in most patients who have had more than 6,000 or 6,500 FUE grafts harvested. Patients with Norwood patterns of hair loss who are going to demand more than 5,500 or 6,000 grafts may be better served with strip harvesting FUT with a trichophytic closure.
Using FUE alone in these large graft count cases may limit the patient’s option to wear his or her hair long. It is very important that we all keep as many techniques as possible in our tool box, integrating techniques if necessary to provide our patients with the best possible result. To quote Martin Unger: “If the only you tool you have is a hammer, everything looks like a nail.”
James Vogel, MD, FISHRS
Over the past 25 years in this field, I have seen many pendulum swings. These swings have created different “camps” supporting or disparaging flaps, reductions, large grafts, small grafts, mixed grafts, trichophytic closure techniques, and, of course, the race to lay claim to performance of the largest graft session to date. However, what ultimately endures are the techniques best suited to provide the optimum results for patient care, not the technique that most satisfies the physician’s ego.
We have all heard the analogy that a hammer is your only tool if that is all that exists in the bag. Certainly not every physician is able to offer all options. However, a practice that does not currently provide both FUE and FUT is unable to meet all patient requirements. Obviously, these requirements range from available donor supply, personal donor styling choices, recipient demand, the patient’s financial resources, and previous scalp procedures, just to name a few.
At the end of the day, a happy patient with a natural appearing result is the only “gold standard” we should promote. Some describe two camps within our specialty: FUE’ers or FUT’ers. However, to think that these represent mutually exclusive options for achieving excellence in hair restoration surgery is naïve and has unfortunate potential to splinter our field.
We should embrace FUE and FUT (strip harvest) as nothing more than two excellent options for donor harvest. The thought process and surgical plan should be what option serves the patient’s needs and leaves physician’s agenda in the waiting room.
- Copyright © 2015 by The International Society of Hair Restoration Surgery
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.