

Abstract
A small number of case reports seem to suggest a relationship between vitamin D deficiency and hair thinning. This article takes a look at the link between vitamin D and hair loss and examines the role of vitamin D in hair growth. Although comprehensive research on the direct link between vitamin D deficiency and hair loss in androgenetic alopecia remains incomplete, this article will discuss what we do know so that you can consider supplementation as a potential medical treatment for hair loss in patients where vitamin D deficiency is identified.
INTRODUCTION
It is well known the hormone DHT (dihydrotestosterone) is etiological to hair loss in genetically affected patients with androgenetic alopecia (AGA). Researchers have shown that each hair follicle is a mini endocrine organ itself that contains receptors and even synthesizes a multitude of different hormones.1 It is not surprising that DHT is only one of many hormones that can impact hair growth or loss. What may surprise some people is the fact that while vitamin D is described as a “conditionally required nutrient,” its designation as a vitamin is something of a misnomer as it is actually considered a steroid hormone.2 While once thought to be mostly involved with calcium and phosphorus metabolism integral to bone health, its range of physiologic effects identified in the past two decades includes a broad swath of immune, neurologic, cardiovascular, and metabolic functions, to name only a few.3 What is important for hair loss specialists to be aware of is the evidence to substantiate its role in normal hair growth and to recognize that the high population incidence of vitamin D deficiency globally may be a contributing factor when evaluating and treating hair loss patients.4,5 Specifically, correction of vitamin D deficiency has been observed in at least two previous published case reports to result in reversal of hair thinning in female patients with no other cause for hair loss.6,7 For decades it has been known that genetic mutations which cause an abnormal vitamin D receptor, usually manifested by various degrees of resistance to vitamin D, often result in alopecia being displayed in affected infants. Research has established the vitamin D receptor as integral to initiating anagen and hair follicle cycling.8 However, the role of vitamin D itself for hair growth has been less clear.
This article represents an additional case report of a patient who presented with a diagnosis of severe vitamin D deficiency and advanced pattern AGA, where the frontal hair was observed to regrow following supplemental treatment and normalization of vitamin D levels. This case report will be followed by a discussion of the relevant literature regarding the important role that vitamin D can play in hair health.
CASE REPORT
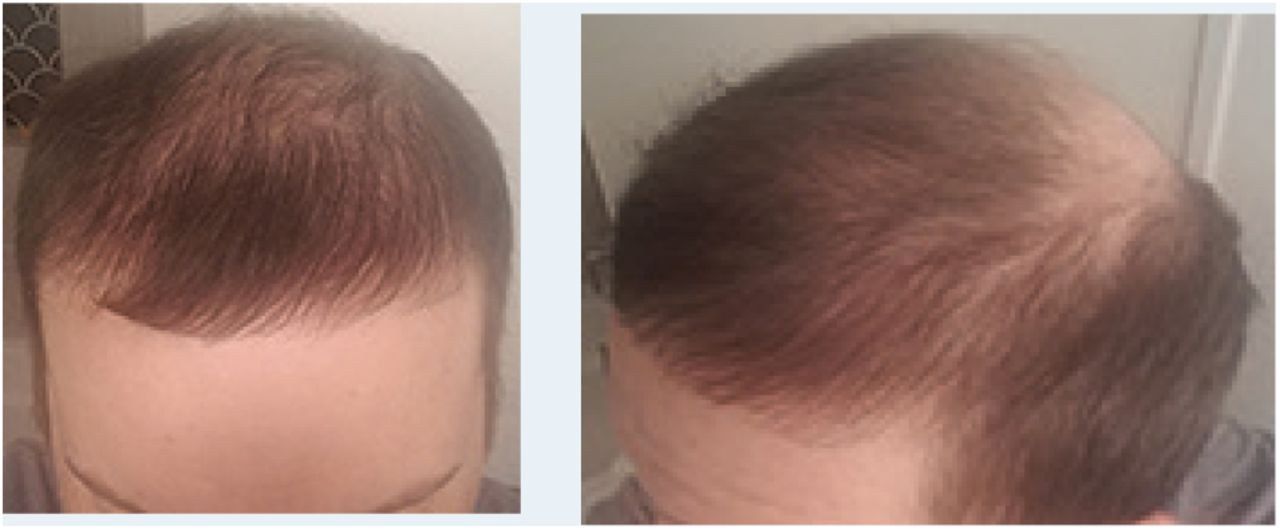
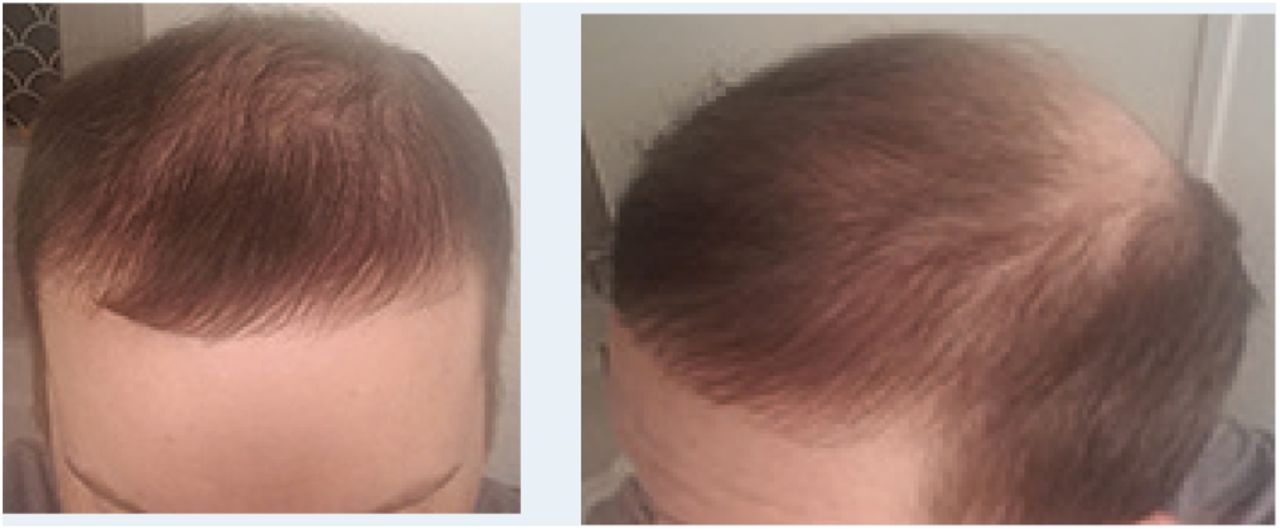
A 41-year-old male patient presented for a virtual consultation to see if he would be eligible for surgical treatment of his patterned hair loss. He had experienced hair thinning since the age of 22, and he had a family history of advanced pattern AGA (maternal uncle Class VI pattern). On review of the patient’s photos, he, too, was observed to have a Class V-VI pattern of hair thinning and hair loss (Figure 1). He had not tried either topical minoxidil or oral finasteride, and he stated his pattern had been stable for 2 years. His past medical history was remarkable for a diagnosis only 6 weeks earlier of severe vitamin D deficiency with a serum 25(OH) vitamin D value of 12ng/ml. He had nearly completed a 6-week course of weekly dosing of 50,000 IU vitamin D3, to be followed by 10,000 IU/week for 8 months. In consideration of this diagnosis as well as the remaining thinning coverage over the frontal area observed in the photos, the patient was educated about the value of medical therapy for AGA-related hair loss as an effort to reverse the miniaturization process in all remaining affected hairs. He was also advised that reducing the size of the affected area of hair loss could reduce the graft numbers needed to achieve his desired cosmetic frontal and crown coverage. The patient stated he was willing to use medical therapy to treat his hair loss. Six months later follow-up photos were remarkable for significant regrowth of frontal hairs (Figure 2). Because he had agreed to begin medical therapy for AGA, it was assumed the regrowth was a response to the medications. Surprisingly, the patient reported that he had decided not to take either finasteride or topical minoxidil and that he had only continued with the vitamin D3 supplements. His serum level of 25(OH) vitamin D at the time of the follow-up had normalized at 50.6ng/ml. He subsequently was seen for an in-person evaluation and was advised not to consider any frontal area grafts because his vitamin D therapy appeared to be achieving effective cosmetic coverage of the frontal area on its own. Since that time, the patient has continued to decline the use of medical therapy to maintain his AGA pattern. He had satisfactory growth from hair transplantation to the vertex area, and one year later he maintained excellent frontal coverage based solely on correction of vitamin D deficiency and has had no further AGA progression to date (Figure 3). This case report supports a diagnosis of non-scarring alopecia in a patient with AGA who experienced reversible frontal thinning caused by vitamin D deficiency and treated with vitamin D3 supplementation.

Thinning coverage (left) and top view class V pattern (right) with early therapy of vitamin D deficiency.
Six months after starting vitamin D supplements treatment, front and side views.

Regrowth at 1 year, front and side views.
DISCUSSION
In addition to the case report presented here, a review of the medical literature regarding hair loss associated with vitamin D deficiency that resolved with supplementation revealed two prior published case reports. The first described a 34-year-old woman with severe deficiency of 25(OH) vitamin D at 12ng/ml, who presented with a 4-year history of progressive, gradual, diffuse hair loss; the patient had normal levels of zinc (Zn), iron (Fe), and thyroid hormones. The second reported the case of a 45-year-old Sudanese woman who had also experienced gradual diffuse hair thinning for 4 years prior to presentation, during which time she reportedly had relocated temporarily to Saudi Arabia and spent most of her time indoors. Her laboratory tests were also normal except for a serum 25(OH) vitamin D level of 9ng/ml consistent with severe deficiency. In both reported cases, treatment with 50,000 IU vitamin D3 for 6 weeks and 3 months, respectively, followed by 1,000 IU/daily as a maintenance dose, resulted in noticeable hair regrowth and resolved the deficiency state. In both cases, the patients received no other topical or systemic treatment. These results lead to the conclusion that these patients share a diagnosis of non-scarring alopecia associated with vitamin D deficiency.6,7
In all three case reports, hair regrowth was associated with supplementation of vitamin D in the absence of other medical or surgical interventions. But if vitamin D deficiency caused hair thinning in these case reports, it begs the questions, does it always cause hair loss? If not, why not, and which patients are at risk for hair loss when vitamin D deficiency occurs? What is the role of vitamin D in hair growth? While these are good questions, research to date does not provide comprehensive answers but the following will touch on what is currently known.
Role of Vitamin D Receptor in Hair Growth
As previously noted, the critical role of vitamin D receptors (VDRs) in normal hair growth is well established by the observed disruption of normal hair growth in many patients with VDR mutations. Animal studies suggest the role of the VDR in the hair cycle is to repress the expression of certain gene(s). The VDR is apparently a negative regulator of a number of genes and the loss of its suppressor activity could potentially lead to the “derepression” or activation of those genes, resulting in alopecia. It is speculated this process may include genes such as the Wnt inhibitor known as SFRP1 (secreted frizzled related protein 1) as well as inhibitors of PTHrP (parathyroid hormone related protein). VDR binding to DNA is a critical function of the VDR in its regulation of the hair cycle. Current understanding is that VDR mutations that cause defects in DNA binding, RXR (retinoic acid receptor) heterodimerization, or absence of the VDR, causealopecia while mutations that solely alter VDR affinity for 1,25(OH)2D3 or disrupt coactivator interactions do not cause alopecia.8 The VDR appears to play an important role in hair follicle cycling by regulating the growth cycle, inducing the development of mature anagen hairs and enabling stem cells in the bulge to replicate. The ligand-independent actions of the VDR would seem to imply that vitamin D is not necessary for the hair growth functions, however, research reveals a strong association between serum levels of 1,25(OH) vitamin D, certain gene polymorphisms, and VDR expression.
To control for gene variations (polymorphisms) in the VDR and vitamin D metabolism, a study in monozygotic twins was performed while studying vitamin D supplementation and its influence on VDR expression. In the study group, supplementation with cholcalciferol (vitamin D3) 2,000 IU × 60 days was found to not only significantly increase serum 25(OH) vitamin D by 65%, but it markedly increased the gene expression of VDR’s as well. Notably, this recent study also found that serum levels of 25(OH) vitamin D > 50ng/dl had other health benefits related to BMI and lean body mass, establishing the health benefits of supplementation beyond previously established low “normal” levels, which averaged 30ng/ml in this study group.9 The VDR is known to be expressed in follicular keratinocytes and dermal papilla cells, and its expression is required for normal hair follicle cycling but apparently not for morphogenesis.10 In view of the impact vitamin D3 supplementation can have on increased VDR expression, it seems possible to anticipate deficiency could adversely impact VDR gene expression in hair follicles and negatively impact their growth cycle.
Multiple Non-Skeletal Functions of Vitamin D
While a causal role for the VDR in hair cycling has been well established, establishing a direct role for hair growth related to the vitamin D hormone itself has been more elusive. The vitamin D hormone is multifunctional in many human organ systems and plays an important role in immune function and regulation, reducing the risk of chronic illnesses, cancer mortality, type 2 diabetes mellitus, autoimmune and infectious diseases, musculoskeletal health, neurocognitive disorders, and cardiovascular and kidney health. More functions are being identified as research continues. For example, researchers have identified 36 tissues possessing the VDR, each with a potential to mount a biologic response to circulating 1,25(OH) vitamin D. The full extent of biologic influence of vitamin D is still under investigation, with researchers estimating vitamin D influences the regulation of more than 1,000 genes within over 20,000 that make up the human genome.11
Evidence for Direct Role of Vitamin D in Hair Growth
In 2016, the first animal study showing a direct association between vitamin D deficiency and hair growth documented a transient loss of hair in nursing pups with a maternal diet deficient in vitamin D and containing low calcium. Alopecia was not present when these pups were suckled by mothers fed with a diet containing calcium and vitamin D. This was the first study to establish a relationship between low calcium and low 1,25(OH) vitamin D and postnatal hair follicle cycling.12 In the past decade, several surveys were performed to assess for a relationship between vitamin D deficiency and certain types of hair loss, some of which appeared to confirm an association between low vitamin D levels and existence and severity of alopecia areata, female pattern hair loss, and telogen effluvium.10,13 Other surveys revealed an association between either high or low levels of vitamin D associated with telogen effluvium suggesting that out of range hormone levels, whether high or low, could stimulate TE.13 A recent survey of 50 young men with early onset AGA compared to 50 age-matched controls confirmed an association between vitamin D deficiency and early onset and severity of AGA.14 However, there apparently has not yet been a published survey of men with documented vitamin D deficiency and AGA to establish the circumstances or percentage of patients likely to achieve some regrowth or reversal of hair loss with treatment and normalization of hormone levels as occurred in this case report.
Cause & Prevalence of Vitamin D Deficiency Globally
For a variety of reasons vitamin D deficiency is reported to have a high prevalence in the global population, with estimates of over 1 billion people affected, including 41% of the U.S. population and 80-90% of people in some middle eastern countries (e.g., UAE). Groups of people at particular risk are those who work indoors, the elderly homebound, those with highly pigmented skin, vegans, and pregnant women, or those who are compulsive about wearing sunscreen when outdoors. Other factors include regions of the world where heat keeps people indoors or clothing norms and fashions cover the body to prevent sun exposure.15,16
Why is vitamin D deficiency so common? As noted, lifestyle, dietary habits, and preferences can make it difficult to obtain enough vitamin D for most people. Few foods naturally contain enough vitamin D to meet daily requirements, though some have been fortified with it to prevent deficiency. Sources of foods rich in naturally occurring vitamin D or commonly fortified include:
Cod liver oil
Salmon
Tuna fish
Swordfish
Sardines
Eel
Caviar or fish roe
Beef Liver
Mushrooms
Egg yolks
Fortified sources (when labeled): milk, orange juice, yogurt, tofu, or cereal
The greatest natural source of vitamin D for humans is vitamin D3 produced in the skin by the action of the sun’s ultraviolet-B rays (UVB) interacting with the provitamin (prohormone), cholecaciferol. Adequate sun exposure can be hampered by living in places where sunlight is limited in winter or where high temperatures encourage people to remain indoors. Furthermore, darker skinned people with higher melanin content in skin require longer periods of time in the sun as the melanin acts like shade to the UVB rays needed to convert the prohormone cholcalciferol, through a series of reactions, to its active hormone, 1,25-dihydroxy vitamin D. For many people, spending sufficient time in the sun to achieve adequate production of vitamin D3 has the undesirable side effect of increasing the risk of damaging effects on the skin, including skin cancer.3 Other causes of deficiency include diseases that inhibit fat absorption (vitamin D is fat soluble) such as Crohn’s disease, celiac disease, or cystic fibrosis. Renal disease may impact the kidneys’ ability to hydroxylate and activate the prohormone, too.15,16
Diagnosis & Treatment of Vitamin D Deficiency
Because of the challenges in obtaining adequate amounts of vitamin D naturally from the sun or through dietary consumption, supplementation orally usually presents a safe alternative. There are two common supplements, vitamin D2 (ergocaclciferol), which is produced in plants and fungi, and vitamin D3 (cholecalciferol), which is produced in animals (including humans). Studies in human subjects have shown vitamin D2 has only one-third the impact on raising serum vitamin D levels compared to vitamin D3, the latter is therefore the preferred supplement.3
Assessment of vitamin D sufficiency requires a simple blood test of 25(OH) vitamin D. The Endocrine Society Clinical Practice Guidelines in 2011 reported 30-100ng/ ml as a desirable range for 25(OH) vitamin D,16 while levels between 21-29ng/ml were considered insufficient, and < 20ng/ml were considered deficient requiring more aggressive correction.11 In each of the case reports reviewed here, the levels were deficient at < 20ng/ml. Over the past two decades, the recommended daily allowance for consumption and supplementation of vitamin D has been changing as documentation of the plethora of important skeletal and non-skeletal functions of this hormone has occurred.17 Many clinical trials have provided evidence supporting serum 25(OH) vitamin D levels > 50nm/ml or 30ng/ml as being associated with greater health benefits.18 Recently, the results of the Harvard VITAL (vitamin D and omega 3 trial) study, a controlled trial of more than 25,000 men and women over the age of 50, evaluated the impact of vitamin D and omega 3 supplementation on cardiovascular disease, diabetes, cancer, autoimmune disease, and overall mortality.19 Pertinent to patients experiencing autoimmune causes of hair loss, adults in the VITAL study supplemented with 2,000 IU/day of vitamin D3 for 5 years exhibited a 22% decrease in autoimmune diseases. Furthermore, when combined with omega 3 supplements there was a 30% reduction in autoimmune disease20—even though both treatment and control groups had a baseline average 25(OH) vitamin D level of nearly 30ng/ml, which was not deficient!21 This suggests health benefits can accrue from supplementation of vitamin D to levels higher than simply being “sufficient.” Furthermore, experts in the field point out that previous recommended daily allowance advisories of <1,000 IU/day were inadequate to treat or adequately reverse levels of insufficiency seen in many populations.22 The Endocrine Society Clinical Practice Guidelines suggests that the maintenance tolerable upper limits (UL) of vitamin D, which is not to be exceeded without medical supervision, is 4,000 IU/d of vitamin D3 for everyone over 8 years and 10,000 IU/d for children and adults 19 years and older when addressing vitamin D deficiency.16 My preferred regimen to treat vitamin D deficiency is the same as that used in the case reports: 50,000 IU vitamin D3 weekly for 6-8 weeks, followed by a serum recheck to assure adequate response. This is subsequently followed by 10,000 IU/week for maintenance, to be adjusted based on serum 25(OH) vitamin D levels.
Avoiding Hypervitaminosis D
If vitamin D sufficiency is so important, and deficiency is so highly prevalent, why not just supplement everyone? As a fat soluble “vitamin,” vitamin D can be stored to levels that cause toxicity. Vitamin D substantially enhances the absorption of calcium and phosphorus in the GI tract. Overabsorption of these elements can result in hypercalcemia and a variety of related symptoms including confusion, abdominal pain, vomiting, polyuria, polydipsia, and dehydration. Levels of (OH) Vitamin D > 150ng/ml are considered toxic. However, in reviewing published literature regarding vitamin D toxicity, data suggests it is relatively difficult to supplement to a level of toxicity with commonly recommended doses of vitamin D. For example, a group of healthy adults receiving 50,000 IU of vitamin D2 every 2 weeks for up to 6 years maintained serum 25(OH) vitamin D levels between 40-60ng/ml and none with evidence of toxicity. (It is notable to recall that Vitamin D2 reportedly has only one-third the ability to increase serum levels of 1,25(OH) vitamin D). Nevertheless, a similar finding was seen in a group of Canadian adults supplemented with up to 20,000 IU vitamin D3 daily for almost a year with no evidence of toxicity (though some had serum levels up to 150ng/ml) as measured and determined by normal serum calcium.23
However, in my own practice where 25(OH) vitamin D levels have now been added to a list of diagnostic tests for hair thinning, a patient was recently found to have an elevated level of 158ng/ml. The patient is an air transport nurse who had been supplementing himself with 4,000 IU daily for the past year after reading about the possible association between low vitamin D and COVID infection severity. He did not check a baseline serum 25(OH) vitamin D level but supplemented empirically according to his recollected “recommended daily allowance.” To identify why his serum levels were so elevated, a dietary history revealed he was a fan of, and frequent consumer of, sardines (canned sardines provide 300 IU vitamin D3/3.5 oz)—one of few foods naturally high in vitamin D. His job also took him outdoors frequently during the day, exposing him to sunlight for extended periods of time. For this patient, dietary consumption and exposure to sunlight were probably sufficient to meet his daily requirements without supplementation. His serum calcium level was normal; however, he had reported a recent increase in hair shedding that began to abate a few weeks after he stopped consuming supplemental vitamin D. This patient’s experience and possible telogen effluvium from hypervitaminosis D underscores the risk of empiric vitamin D supplementation in favor of a baseline serum measurement, with appropriate supplementation only if deficient, and follow-up measurements to establish a healthy steady state.
CONCLUSION
Specialists in the field of hair loss treatment have in recent years published advisories to recommend serum 25(OH) vitamin D levels be routinely checked in hair loss patients as vitamin D deficiency represents a common clinical entity where treatment has the potential to improve or even reverse various types of hair loss.4 This case report of a male patient with AGA revealed substantial reversal of hair loss with treatment of severe vitamin D deficiency. Prior to meeting the patient in this case report, measuring 25(OH) vitamin D levels was not a routine lab test for my patients. Had this patient not already been diagnosed and prescribed treatment for vitamin D deficiency, how might his clinical course in my hands have been different? It is a disconcerting thought. I now routinely advise patients to check for and treat vitamin D deficiency along with any other recommended hair loss therapies that I usually suggest. The question remains to what degree vitamin D deficiency is a direct cause of hair loss or whether it is the impact it has on the gene expression of VDRs or related to a myriad of other genetic regulatory influences of vitamin D that have yet to be fully elucidated. Regardless of whether the impact of vitamin D deficiency is a direct or indirect contributing factor for hair loss, the solution for most patients who are vitamin D deficient is simple enough: oral supplements with vitamin D3 to achieve and maintain a serum level of 25(OH) vitamin D between 40-100ng/ml (the lower limit reflecting the average serum levels in the VITAL treatment group after 1 year) with periodic blood sampling to assure against overzealous supplementation and hypervitaminosis D.
- Copyright © 2022 by the International Society of Hair Restoration Surgery
This article is open access and may not be copied, distributed, or modified without written permission from the International Society of Hair Restoration Surgery.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.