

Abstract
Alopecia areata (AA), with a disease incidence of 2% in the USA, is the most common immune-mediated cause of hair loss in the world. There were no FDA approved treatments for AA in the past. All treatment modalities used alone or in combination with each other, were prescribed off label. The JAK inhibitor baricitinib was approved by the FDA in June 2022. While it’s a significant leap forward, we are still missing the safety profile data in multiple areas. Topical JAK inhibitors are being tested along with sublingual options including tofacitinib, ruxolitinib, and ritlecitinib. In this review, we discuss the JAK inhibitor baricitinib in detail, along with its dosing regimen, challenges presented in the clinic, missing data, and what the future may hold.
INTRODUCTION
Alopecia areata (AA) is the most common immune mediated cause of hair loss in the world.1,2 The disease incidence in the USA and United Kingdom is approximately 2%.3 AA affects both children and adults and does not show a preference for gender, skin type, hair type, or hair color.2 AA is characterized by a circular well-circumscribed area of hair loss, typically on the scalp or face, but it can affect any hair-bearing region.1,2 It can range in severity from patchy, diffuse involvement to more severe forms involving the entire scalp or all body hair. AA can be a self-limiting condition that often results in spontaneous regrowth, but as an autoimmune disease, disease extent and activity can vary and patients can experience recurrent episodes of patchy or extensive hair loss.1,3,4 While the disease mechanisms driving AA have not been fully determined, it is clear that genetic predisposition and autoimmunity are key contributors together with likely environmental factors.3 Genetic epidemiology has demonstrated an increased risk of AA in first degree relatives, with the incidence being between 10% and 50%.1,3,5 This genetic predisposition has been linked to the major histocompatibility complex (MHC) gene and more specifically to the human leukocyte antigen (HLA) class II genes.1,3,5 Many single nucleotide polymorphisms (SNPs) associated with AA led to the identification of candidate susceptibility genes through genome-wide association studies (GWASs).1,3,5 Previous studies showed that AA largely involves attack of the hair follicle bulb region by autoreactive CD8+ T-cells, which comprise the characteristic “swarm of bees” around the hair follicle bulb in AA. These autoreactive T-cells are initially activated by numerous cytokine pathways that utilize the Janus kinase (JAK)-signal transducer and activator of transcription (STAT) signaling.1-4 Treatment of AA has been challenging in the past due to an inadequate understanding of the pathogenesis of the disease.6
Past and Current Treatments for AA
Current treatment strategies for patients with AA differ based on several factors including disease severity, affected area(s), and patient age. Broadly, these can be categorized into three groups: topical, intra-lesional, and systemic therapies.
Traditional first-line therapies for patients with limited AA include topical (TCs) and intralesional corticosteroids (ICs). For both children and adults, use of higher potency TCs is preferred as they have been shown to be more effective than lower potency TCs.7 Concurrent therapy with topical minoxidil has also been described in the literature, but its efficacy is restricted to patients with limited or patchy AA.8 Other topical therapies include anthralin 0.5-1%, a contact irritant that is occasionally used as a second- or third-line agent for the treatment of limited or diffuse disease.5 As with other AA treatments, patient response is variable, and there is a high rate of recurrence following cessation of therapy.
For patients with diffuse or recalcitrant AA, contact immunotherapy with diphenylcyclopropenone (DPCP) or squaric acid dibutyl ester (SADBE) is a leading treatment modality. Following initial sensitization, DPCP or SADBE is applied at increasing concentrations until a mild contact dermatitis occurs after which treatment frequency is based on patient response. In a meta-analysis across patients with varying degrees of AA, 32% of patients treated with contact immunotherapy experienced complete regrowth, with 49% of these patients relapsing after treatment discontinuation.9
Systemic therapies, such as systemic corticosteroids (SCs), systemic immunosuppressive agents, and Janus-kinase inhibitors (JAK-inhibitors), are usually reserved for treatment of severe, recalcitrant AA as in alopecia totalis and alopecia universalis. SCs are often prescribed as acute rescue therapy in cases of rapid, widespread hair loss in an effort to slow the rate of disease progression while simultaneously stimulating hair regrowth.5,10 Though efficacious in this aspect, their long-term use is contraindicated due to the potential for negative side effects, and patients are typically placed on alternate therapy once disease activity has stabilized.
Methotrexate and cyclosporine are systemic immunosuppressive agents that have shown efficacy in stimulating hair regrowth in patients with AA. In a meta-analysis by Phan et al methotrexate was found to stimulate complete hair regrowth in 63.3% of AA patients. Combination therapy of methotrexate with SCs was found to improve this growth response.11 Data on cyclosporine use in AA is sparse, likely given its adverse effect profile that limits its ability to be used long term. As with SC use, when using systemic immunosuppressants, patients have to be carefully monitored for any adverse side effects and long-term use of cyclosporine is contraindicated.5,12
Until recently, there was no FDA-approved therapy for the treatment of AA.
JAK Kinase Signaling
Within the field of dermatology, JAK-inhibitors represent a new class of focused therapies for the treatment of several autoimmune and inflammatory disorders, including atopic dermatitis, psoriasis, vitiligo, and most recently AA.
The JAK-STAT signaling pathway mediates a wide variety of cellular processes including inflammatory responses, leukocyte maturation, and recognition of microbes, among others. Many cytokines and hormones, such as IL-2, IL-4, IL-5, IL-13, IFN-y, erythropoietin, thrombopoietin, and GM-CSF, activate the JAK-STAT pathway.13 The JAK family includes JAK1, JAK2, JAK3, and TYK2; the STAT family includes STAT1, STAT2, STAT3, STAT4, STAT5a, STAT5b, and STAT6. Upon ligand binding, JAKs become activated and mediate signal transduction that phosphorylates STAT transcription factors. When phosphorylated, STATs dimerize and translocate to the nucleus to bind to DNA to affect gene expression.14 When various type I and II cytokines bind to their receptor subunits, such as type 1 IFNs, IL-6, IL-12, or IL-23, specific downstream intracellular JAK signals are activated that play important roles in the pathogenesis of immune diseases.15 Furthermore, the IL-6-activated JAKs interact with other activated cytokine-mediated signaling pathways, therefore, blockade of the JAK-STAT pathway inhibits many downstream immune responses.
The pathogenesis of AA involves inflammation around the hair bulb that is mediated by IFN-γ and IL-15, which in turn activate CD8+ T-cells via the JAK-STAT pathway, suggesting that JAK inhibition may be an effective treatment option for AA.13,16 In transcriptional profiling of AA lesional skin from both C3H/HeJ mice and AA patients, gene expression signatures showed pathways consistent with cytotoxic T-cell infiltration, known to promote IFN-y producing CD8+ T-cells.17 To validate these findings, it was shown that antibody-mediated blocking of IFN-y, IL-2, or IL-15RB prevented the development of disease and decreased the accumulation of CD8+ T-cells in the skin and the dermal IFN response in the AA mouse model. In preclinical studies using JAK inhibitors in C3H/HeJ mice, hair regrowth was observed using several different JAK inhibitors, such as tofacitinib, ruxolitinib, and baricitinib.17 JAK inhibitors administered systematically reduced the IFN signature and prevented AA development, while topically administered treatment promoted hair regrowth in mice that had long-standing AA.17 These proof-of-concept studies in C3H/HeJ mice provided a strong rationale to test these medications in humans.
The first case reports to emerge showed dramatic clinical responses in AA patients treated with ruxolitinib and tofacitinib.17,18 These were replicated in the literature with numerous other case series of patients showing significant hair regrowth and improvement in AA. Several open-label studies followed, in which extensive hair regrowth was observed using ruxolitinib and tofacitinib, which showed impressive patient responses.19-22 In one study, 12 patients with moderate-to-severe AA used oral ruxolitinib 20mg twice per day for 3-6 months with 9 patients showing an impressive response to treatment, averaging 92% of hair regrowth, with no serious adverse effects reported.22 In a second study, 11 of 12 patients showed global improvement in Severity of Alopecia Tool (SALT) score after receiving and tolerating oral tofacitinib 10mg twice a day, with 1 patient showing improvement at the 5mg dose twice daily and 1 patient discontinuing the study due to hypertension.21
In larger open-label studies, 66 patients were treated with oral 5mg tofacitinib twice daily for 3 months resulting in 32% experiencing 50% or greater improvement in the SALT score.20 Although the dose and duration of tofacitinib was both safe and effective, durable responses were infrequent, and drug cessation resulted in disease relapse in about 8.5 weeks. Another report retrospectively studied 90 patients treated with tofacitinib, of which 65 were potential responders to therapy, demonstrating a 77% clinical response without reports of serious adverse effects.23
Several JAK inhibitors are currently under clinical investigation, as described below.
FDA Approval of Baricitinib for AA
In June 2022, baricitinib became the first JAK inhibitor to achieve FDA approval for the treatment of AA in the United States. Baricitinib is an oral selective and reversible competitive inhibitor of JAK1/2 that was originally approved in 2018 for the treatment of moderate to severe active rheumatoid arthritis.24 More recently, in 2021, baricitinib was approved for treatment of COVID-19 in hospitalized patients.25,26
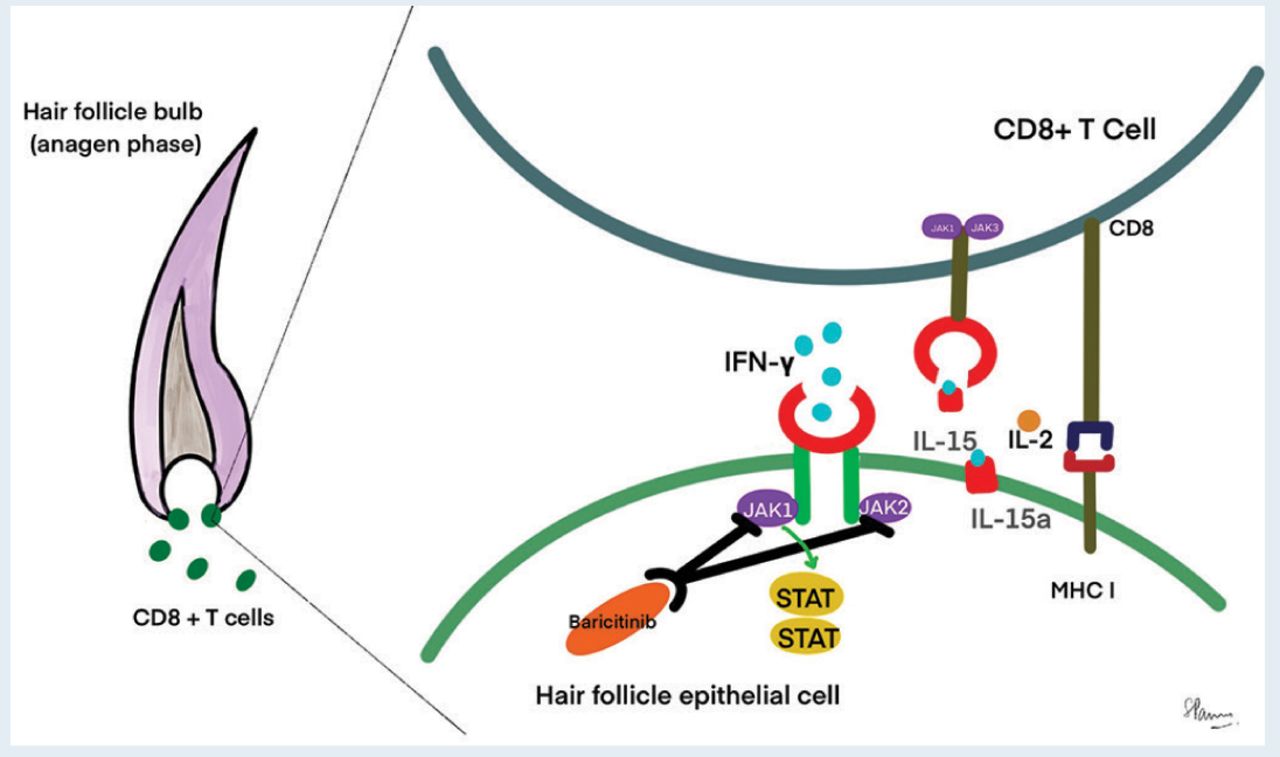
Baricitinib blocks the intracellular transduction of STAT proteins that modulate the signaling pathways downstream of various interleukins, interferons, and growth factors. CD8+ T-cells produce IFN-γ, which signals via JAK1/2 to enhance IL-15 production. After binding to IL-15a (chaperone protein), IL- 15 binds to the surface of CD8+ T-cells and activates more IFN-γ production through JAK1/3 signaling. Baricitinib blocks JAK1/2-mediated signaling pathways, thereby ameliorating the immune response around the hair follicle (Figure 1).19
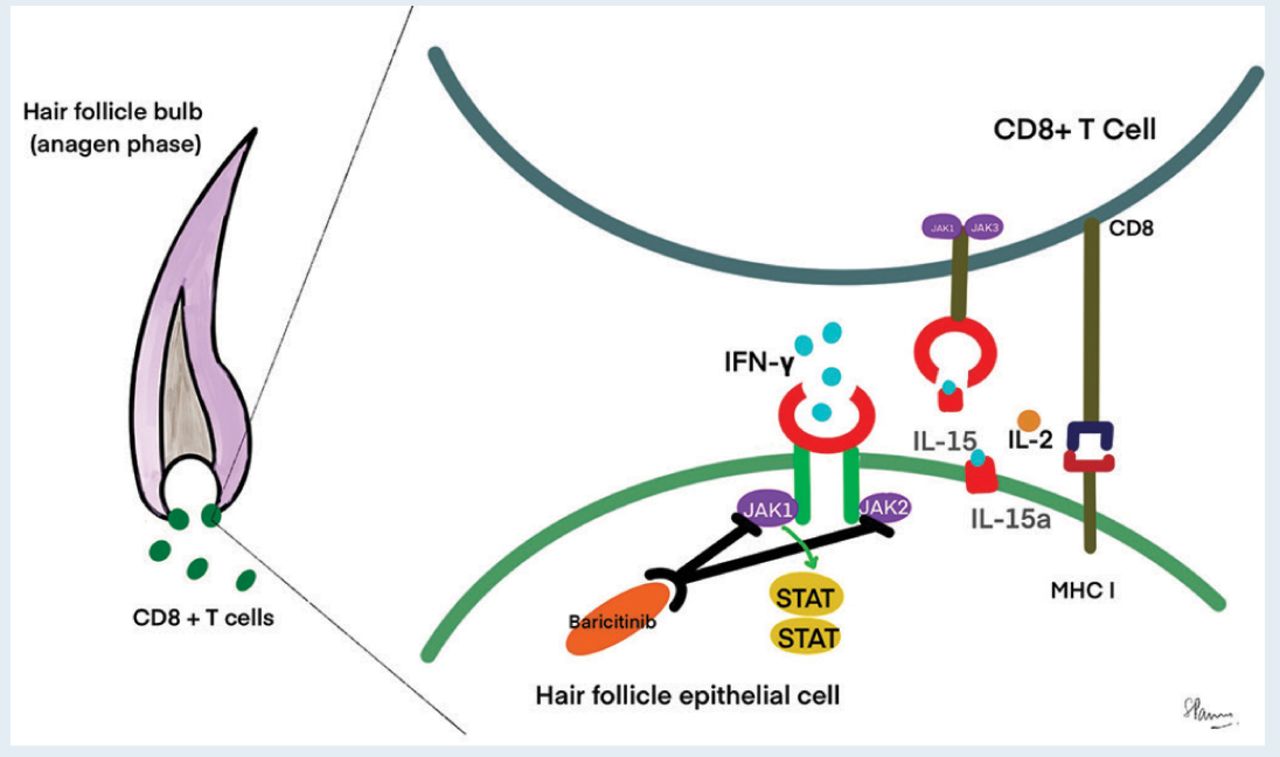
Baricitinib blocks JAK 1/2 mediated signaling pathway resulting in decreased IFN-y downstream. This ameliorates the immune response around the hair follicle.
The efficacy and safety of baricitinib was studied in two large 36-week randomized, double-blind, placebo-controlled phase 3 trials. BRAVE-AA1 trial enrolled 654 patients and BRAVE-AA2 enrolled 546 patients. The selection criteria were male (18-60 years) and female (18-70 years) AA patients with SALT score of 50 or higher and a duration of the current episode of alopecia between 6 months and 8 years. SALT score of 20 or less was considered significant improvement in patients with AA. SALT of 20 or less was the primary outcome of the trial at week 36 for patients on once daily 4mg baricitinib and 2mg baricitinib.27 In March 2020, the U.S. FDA granted breakthrough therapy designation to baricitinib for treatment of AA and granted approval in June 2022.28
Dosing and Safety Considerations
The BRAVE-AA1 and BRAVE-AA2 trials used 4mg and 2mg oral baricitinib twice daily.27 However, the FDA approved 4mg once daily dosing in patients with AA. Baricitinib must be taken orally, with or without food at any time during the day. If the patient is > 75 years of age, then a 2mg once daily dosing is advised. In the cases where desirable results have been achieved, the dosing can be tapered to 2mg once daily from 4mg once daily baricitinib. It is recommended to continue the drug for several months after the results are achieved to prevent the chances of relapse.
Baricitinib is mainly excreted via the kidneys (75%) and gut (20%). Only 10% is metabolized by oxidation with CYP3A4 enzymes. Dose should be reduced in patients with compromised GFR. The recommended dose for patients with creatinine clearance between 30 and 60ml/min is 2mg baricitinib. It is contraindicated in patients with GFR less than 30ml/min. It is not recommended in patients with severe hepatic impairment.29
Baricitinib increases the risk of infections in patients, most notably upper respiratory infections. It may also be associated with the reactivation of TB and viral infections like herpes zoster. Hence, patients should be screened for any past or current infections and immunocompromised states since this drug is an immunosuppressant. It may also increase the risk of malignancies and especially lymphoma. Baricitinib may cause thrombosis and must be used with caution in patients with deep vein thrombosis (DVT) and pulmonary embolism (PE). Baricitinib may also cause diverticulitis and gastrointestinal perforations. It may be excreted in breast milk and must not be used during lactation or breast feeding. In clinical trials, acne was one of the most common adverse events. Acne has also been reported with other JAK inhibitors like tofacitinib, which was used extensively off-label for the treatment of AA.30 Baricitinib carries a black box warning for cardiovascular events especially in patients over 50 years of age with at least one heart disease risk factor and a history of smoking.
Clinical data are still emerging in the treatment of pediatric alopecia areata, and long-term effects on fertility, pregnancy, and teratogenic potential are unknown. The ongoing long-term safety evaluations are a step forward toward resolving these unanswered questions.24
The Future of JAK Inhibitors in AA
The future therapeutic applications of the JAK inhibitors appear promising. They have shown wide-ranging efficacy across a number of autoimmune and inflammatory skin diseases, including vitiligo, psoriasis, and atopic dermatitis as well as AA. Concurrent with the success of oral JAK inhibitors, topical JAK kinase inhibitors for AA have also garnered interest. In 2017, a small clinical trial in 6 pediatric patients using topical 1% and 2% tofacitinib or ruxolitinib ointment showed mild improvements in scalp, eyebrow, and eyelash hair.31 The topical formulations were overall well tolerated with minimal side effects. However, it was noted that different drug delivery vehicles affected the clinical outcomes in reports of topical JAK inhibitors, and those that were compounded in a liposomal base versus VersaBase cream (non-liposomal base) provided better efficacy.31 Another double-blind, randomized, vehicle-controlled phase 2 study was conducted following an open-label study of 1.5% Ruxolitinib cream for AA, however, no significant improvement was determined.32 Similarly, a trial with delgocitinib ointment 30mg/g for 12 weeks did not show statistically significant results in SALT improvement.
These failures were attributed to the inability of the topically delivered drugs to penetrate deep enough to reach the perifollicular inflammation.33 In a pilot clinical trial, sublingual tofacitinib was used to treat AA. Sublingual tofacitinib bypasses the hepatic first pass, increasing bioavailability and enabling once daily dosing due to 11 hours long half-life. A SALT50 was achieved by only 12.5% patients.34 Tofacinitib has been combined with other medications to stimulate hair growth, including steroids, topical minoxidil, and oral minoxidil, though the synergy of these medications, if any, is unknown.
Currently, several additional clinical trials are in progress using other JAK inhibitors. A clinical trial of CTP-543 (a deuterated form of the JAK1/2 inhibitor ruxolitinib from Concert Pharmaceuticals) has reported that 41.5% patients in 12mg BID dose and 29.6% patients in 8mg BID dose achieved SALT of 20 or less (REF). Ritlecitinib (a covalent a JAK3/TEK inhibitor from Pfizer) is in ongoing clinical trials in AA and has shown promise in pediatric alopecia areata.35 Jaktinib (a pan-JAK inhibitor from Zelgen Pharmaceuticals) is in ongoing clinical trials for AA. The future of JAK-inhibitor drug development for AA is robust, and it is expected that topical formulations with improved penetration will soon be on the horizon.
CONCLUSION
With baricitinib being approved by the FDA as a new treatment modality for AA, we have ushered into a new era of targeted therapy. Yet many questions remain unanswered, such as safety profile data on malignancies, hepatic side effects, and drug interactions, among others. Additionally, data on the impact of baricitinib on fertility and teratogenic effects is missing, and currently, baricitinib is contraindicated in pregnancy. Animal studies have shown a possible impact on female fertility, but no impact on male spermatogenesis has been demonstrated.24 Additional studies are needed to assess the safety and efficacy of JAK inhibitors in pediatric populations. Though the future looks promising for JAK inhibitors in AA, understanding their long-term safety profile is pertinent to their ultimate success.
- Copyright © 2022 by the International Society of Hair Restoration Surgery
This article is open access and may not be copied, distributed, or modified without written permission from the International Society of Hair Restoration Surgery.
References
In this issue





{kind=link}
Related Articles
Cited By...
- No citing articles found.