
Optimal patient selection for hair transplant procedures is one of the elements of a correctly carried out reconstructive scalp treatment. Appropriate quality of the donor site is a fundamental prerequisite to achieve the necessary number of grafts and guarantee good hair growth in the recipient area. It is particularly important to determine the degree of miniaturization in the recipient area as well as to define the ratio of anagen and telogen hairs. Too high a number of vellus hairs indicates a clearly intensified miniaturization process, which slowly evolves into lack of hair growth and, with time, hair loss. Similar conclusions may be drawn if the number of telogen hairs is increased. Also evaluation of donor sites may be useful in correct patient selection for hair transplant procedures. Considerable miniaturization observed in this area should alert the surgeon to opt for conservative treatment, using finasteride as a sole treatment or as support to surgical intervention.
So far the most frequently used methods of scalp evaluation in both donor and recipient areas have been the following: non-invasive methods such as visual evaluation (macroscopic test),2 evaluation with a microcamera, and visual analysis of magnified images—phototrichogram,3-7; semi-invasive methods such as a trichogram8,9 with microsopic analysis of hairs plucked from a selected scalp area; and invasive methods10,11 such as scalp biopsy. All these techniques, albeit effective, have a fundamental shortcoming, namely their precision is totally dependent on the experience, perceptiveness, and conscientiousness of the examiner. Thus, we may categorize them as subjective, that is, man-dependent evaluation methods.
A technique, which combines excellent optics with computer analysis, is the TrichoScan.12 The method, as described by Rolf Hoffmann, makes use of computer processing of standard epiluminescent camera (ELM) images. This method makes it possible to objectively assess in situ such hair growth parameters as the following:
Hair density (n/cm2)
Hair diameter (um)
Hair growth rate (mm/day)
Ratio of anagen to telogen hairs
Ratio of miniaturized to terminal hairs
TrichoScan is an objective test, not relying on human accuracy, that can be applied in the diagnosis of hair loss processes and in efficacy studies of various medications and laser treatments. In addition, it can be used to assess the effectiveness of surgical treatment. TrichoScan may also prove extremely useful in selecting patients for hair transplant procedures.
Objective
The aim of the study was to compare three different methods of evaluating the donor site in patients with androgenetic alopecia (AGA) undergoing hair restoration surgery (HRS). Hair density (HD) (hair number/cm2) and miniaturization grade (MG) (vellus/terminal hair ratio) were the parameters to be measured. The evaluation methods compared were: 1) macroscopic examination; 2) videomicroscopy; and 3) the TrichoScan method.
Materials and Methods
Forty patients (both males and females) with AGA (ages 20–51 years) were included in the study. The patients were divided into four age groups: 20–30 years (10 men), 31–40 years (10 men), older than 41 (10 men), and 10 women aged 25–45 years. A 1.8cm2 area was chosen at the occiput of the donor area and was evaluated by two independent investigators. The following techniques were compared to determine the variability of results between the two investigators: macroscopic examination (manual counting of hair); videomicroscopy combined with Mirror (Canfield Imaging System) analysis; and the TrichoScan method (Fotofinder DERMA, Teachscreen Software, Bad Bimbach, Germany). Each examiner worked separately and statistical analysis was performed using the one-sample t-test.
The hair in the donor site was shaved to the length of 1 mm.
In the macroscopic method only hair density (HD) was determined using a four-grade scale as follows:
- Insufficient
- Sufficient
- Good
- Very good
Macroscopic MG was not measured due to the high risk of error associated with naked eye perception devoid of optical instruments.
In the videomicrosopy examination a photograph was taken of the area under study using a micro-VID digital hand-held microscope. The photograph was subsequently analyzed using the Mirror Program. The default setting of this system to count hairs was modified in the following way: a single click marked as “1” signified a miniaturized hair (vellus) and a double click marked as “2” stood for a terminal hair. By comparing the ratio of 1 to 2, the MG was determined.
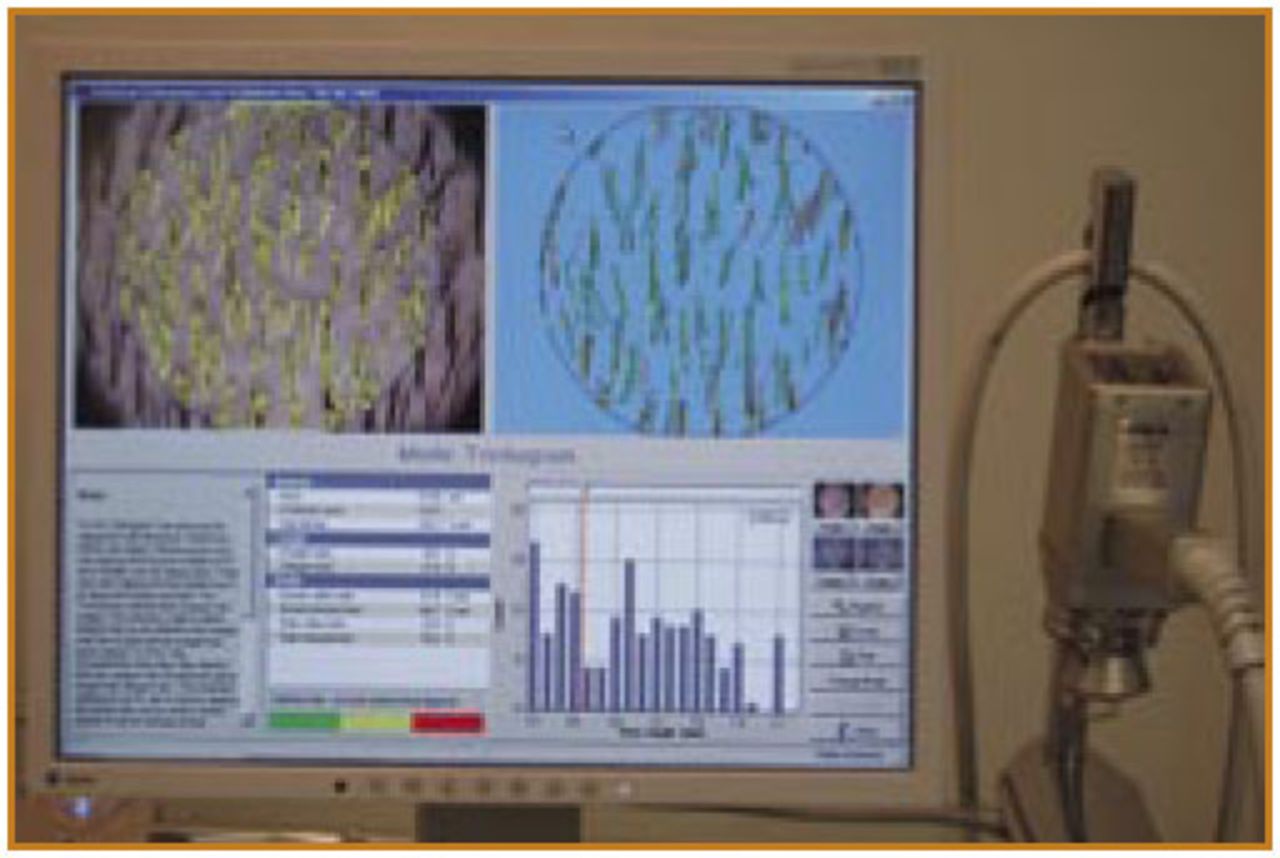
For the TrichoScan method, the area under study was dyed a dark color (Figure 1). The dye was left on for 12 minutes and was removed with an alcohol solution. A photograph was then taken with an epiluminescent camera. The photographed area remained wet throughout the examination and the proper distance between the camera and skin surface was maintained by a rigid contact lens (Figure 2). The image was processed by the software, which followed defined algorithms to allow for assessment of, among other parameters, HD, which was expressed in n/mm2, and MG, which was expressed as a percentage of vellus hair to terminal hair. The results were presented graphically and digitally (Figure 3).



Results
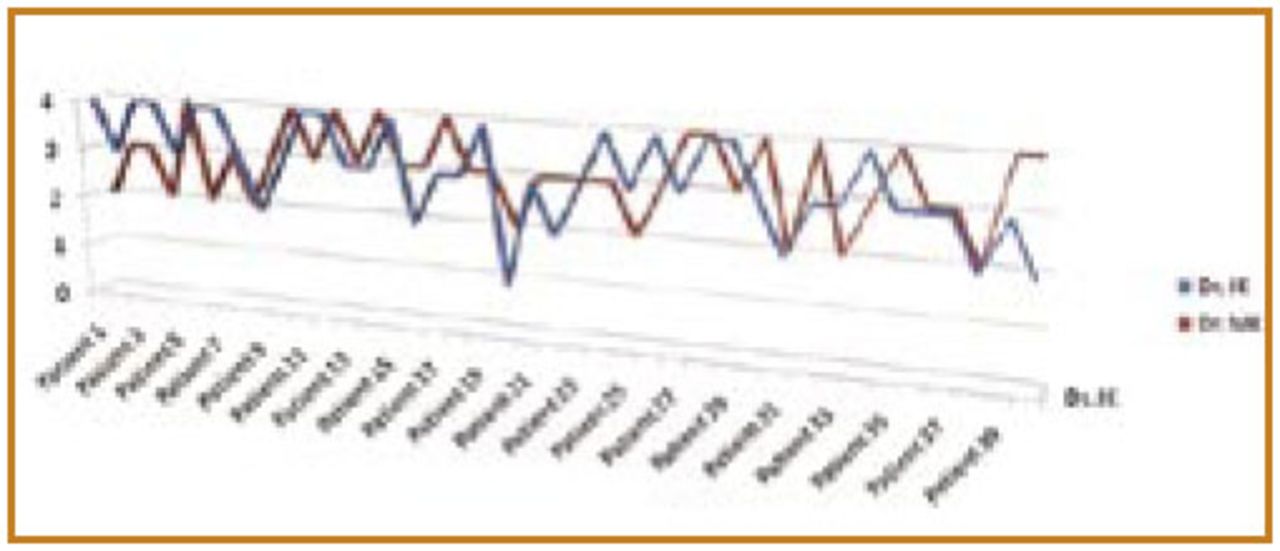
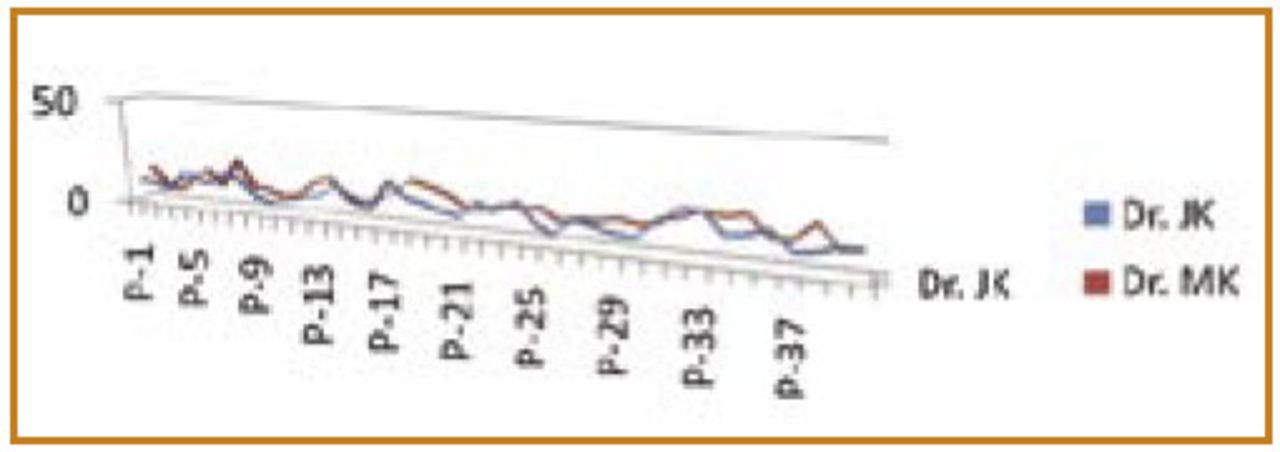
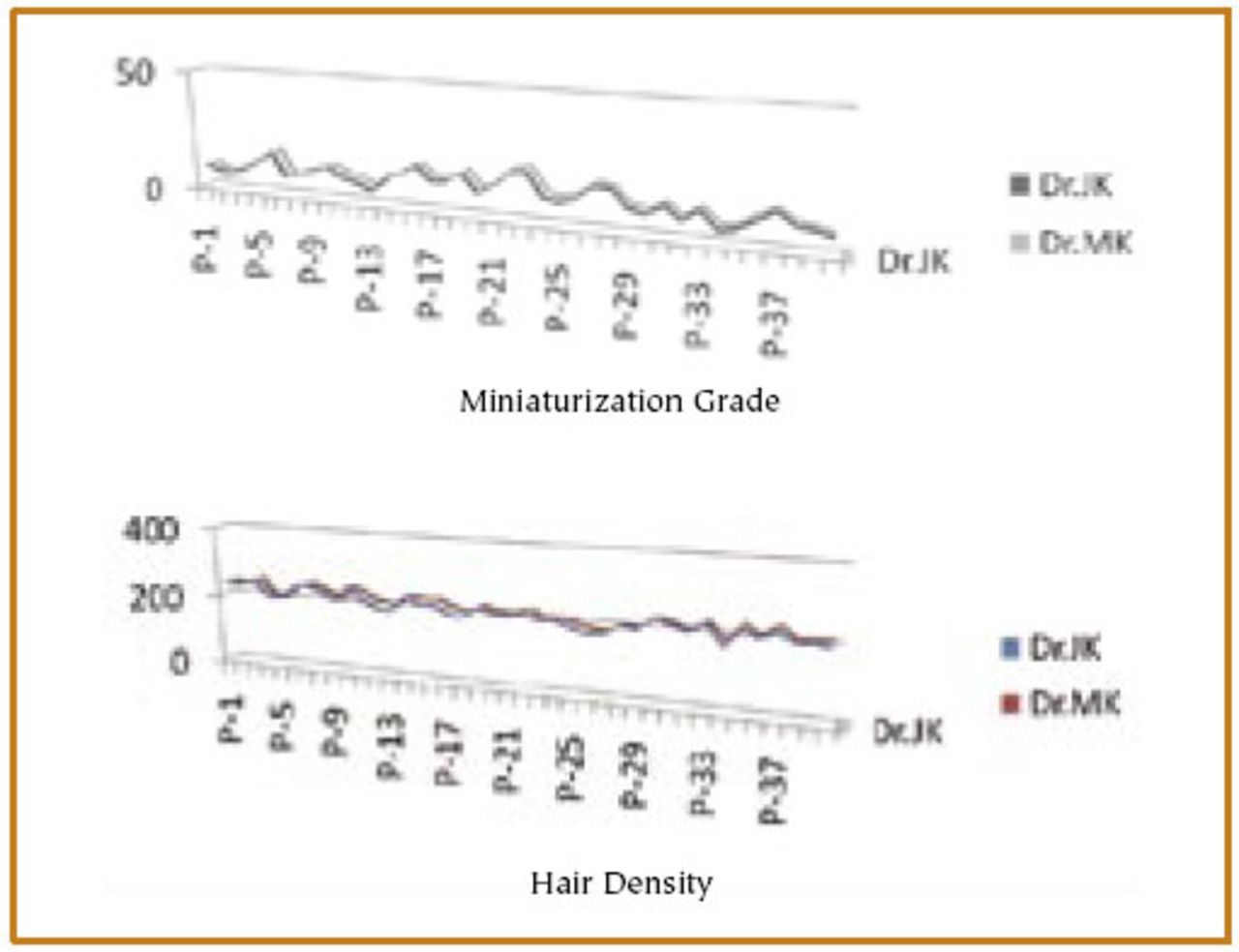
Using the rough macroscopic examination with the 4 grade scale to measure HD, the differences between two experienced investigators were statistically significant (Figure 4). With videomicroscopy, there were clear differences in respect to both HD and MG measurements (Figure 5), although only the MG difference was statistically significant. The results rendered by the TrichoScan method were surprisingly uniform as there was practically no difference between the two examiners (Figure 6). Moreover, the calculated correlation (ANOVA) between the investigators in respect to both HD and MG was more than 97% and 95%, respectively.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
The most frequent indication for hair transplantation is AGA, which is characterized by intensifying hair miniaturization. This process initially affects individual hairs within the follicular unit.13 In that period, the overall number of hairs per square centimeter may remain unchanged. Gradually, however, the number of miniaturized hairs within follicular units increases, leading to macroscopically observed scalp skin visibility, which is the first and most basic symptom perceived by patients.
Early diagnosis of hair miniaturization makes it possible to start early medical therapy.14 Evaluation of hair density and degree of miniaturization are of fundamental significance in selecting patients for hair transplant procedures.13 Miniaturization that is too intensified may result in unsatisfactory regrowth of transplanted hair.15,16 Pre-operatively, determination of hair density in the donor site makes it possible to precisely calculate the strip width necessary. So far most methods used for evaluation of HD and MG in the donor site have been subjective and correlate to the “accuracy of the eye” of the examiner. The TrichoScan method is the first objective method for examination of human scalp that does not rely on human accuracy.12 It enables evaluation of both hair density as well as miniaturization grade in the examined site. If the test is repeated three days after trimming the hair in the area under study to 1mm in length, it is possible to determine the ratio of anagen to telogen hairs (the anagen hairs grow in length).
The TrichoScan method is a useful tool in the diagnosis of alopecia processes and in objective monitoring of various methods of conservative treatment. Our results have shown that this test enables an objective examination of HD and MG, which plays an important role in selecting patients for hair transplant procedures.
Because in using the TrichoScan method the hair at the donor site is dyed prior to the digital analysis, the precision of vellus hair detection was almost 100% (all vellus hair between 5 and 40μm will be detected with this method). Thus, it was possible for us to establish an approximate cut-off for optimal donor site parameters in hair transplant candidates. MG lower than 10% was considered a sign of a steady donor region that would render the best HRS result.13 Values between 10-15% at the donor site were considered borderline and might result in an unsteady surgical outcome if the trend continued. MG over 15% at the donor site was considered an ominous sign, especially in younger patients (less than 25 years old), and an indication that surgery should not be attempted.
The accuracy and clear visualization of results with the TrichoScan also make for much better communication between doctor and patient. This is especially important in managing patients younger than 25 years of age. This test also makes it possible to precisely diagnose diffuse patterned and unpatterned alopecia. Digital and graphic visualization of test results helps patients better understand the structure of their scalp and degree of its loss as well as the type of recommended treatment. Thus, patients are more actively involved in the process of diagnosis, management, and evaluation of results. These studies have shown the objective nature of this test. In my opinion, TrichoScan should be considered as a basic tool in the process of the evaluation of medical and surgical treatment of hair loss patients.
Conclusion
Using TrichoScan for a pre-operative donor site evaluation greatly enhances patient selection for hair restoration surgery. It is a new tool that provides objective and fully reproducible information in regard to measuring hair density and miniaturization grade. It is especially useful in diagnostically difficult cases.
Editors’ note: The TrichoScan device can be purchased from Fotofinder DERMA, Teachscreen Software, Bad Bimbach, Germany. The price is about US$15,000. More information can be found at www.trichoscan.com. To the author’s knowledge, the company doesn’t provide initial training. The ISHRS Regional Workshop in Poznan, Poland, will provide the opportunity for training exposure to this technology. You can preview the workshop program at www.ishrs-chopin.pl.
Footnotes
* The author has no financial interests or commercial associations that might pose or create a conflict of interest with the information presented in this article.
- Copyright © 2009 by The International Society of Hair Restoration Surgery
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.