
Female pattern hair loss…to treat or not to treat? And with what? Does anything really work for women?
Many in our field would argue that it’s not worth even treating women, citing concerns about donor area, the paucity of effective treatments, or how it can be difficult or impossible to achieve patient satisfaction. But these concerns should not prompt us to give up. Rather, women can be some of the most rewarding patients to treat, and using simple things like handouts, dermoscopy, and photography can help increase understanding, reduce confusion, increase compliance, and dramatically improve their response to treatment.
Women often undergo an extensive workup before arriving at a diagnosis of FPHL. They may start by seeing their internist, then their OB/GYN, then their endocrinologist, and even a naturopath before seeing a dermatologist or hair loss specialist. Along the way, they may get told that the hair loss is due to stress, adrenal fatigue, or “low-normal” thyroid function, all of which when corrected fails to stop the hair loss—until they find YOU! In a matter of seconds, you recognize the presence of miniaturized hairs either on clinical examination or with the use of dermoscopy. Finally, they get the diagnosis they have been dreading: female pattern hair loss. They believe nothing can be done for them…or can it?
Although there is only one FDA-approved medication for hair loss in women (topical minoxidil), there are other off-label options such as oral spironolactone, oral finasteride, and certain birth control pills that can be tried before or in addition to hair transplantation. Women may also benefit from low level light therapy (LLLT), which has 510K FDA clearance as a medical device. Depending on how advanced their degree of hair loss, they may benefit from one or more therapies. The physician should consider their comorbidities, lifestyle, family planning, and personal preferences.
Topical Minoxidil
The only FDA-approved medication for hair loss in women is topical minoxidil or Rogaine®. There is new evidence that use of topical minoxidil can improve the quality of life with FPHL.1 The drug is recommended for twice daily usage as a 2% solution for women and as a 5% foam and solution for men. The 2% solution has been shown to be effective at arresting hair loss in 60% of cases,2 and even better results have been seen with the 5%.3 Excellent results can be achieved with consistent usage (Figure 1). Recently, one study showed that the 5% foam worked just as well, used once daily in women, as the 2% worked twice daily.4 There also were fewer complaints about pruritus and dandruff. Many physicians already recommend using the 5% foam once daily at bedtime as a way to increase compliance and simplify the morning grooming routine. This has since prompted the FDA to approve a women’s 5% Rogaine foam formulation for once daily usage.5 The risk of hypertrichosis should still be discussed as it has been reported in 8.9% of patients using this regimen.6

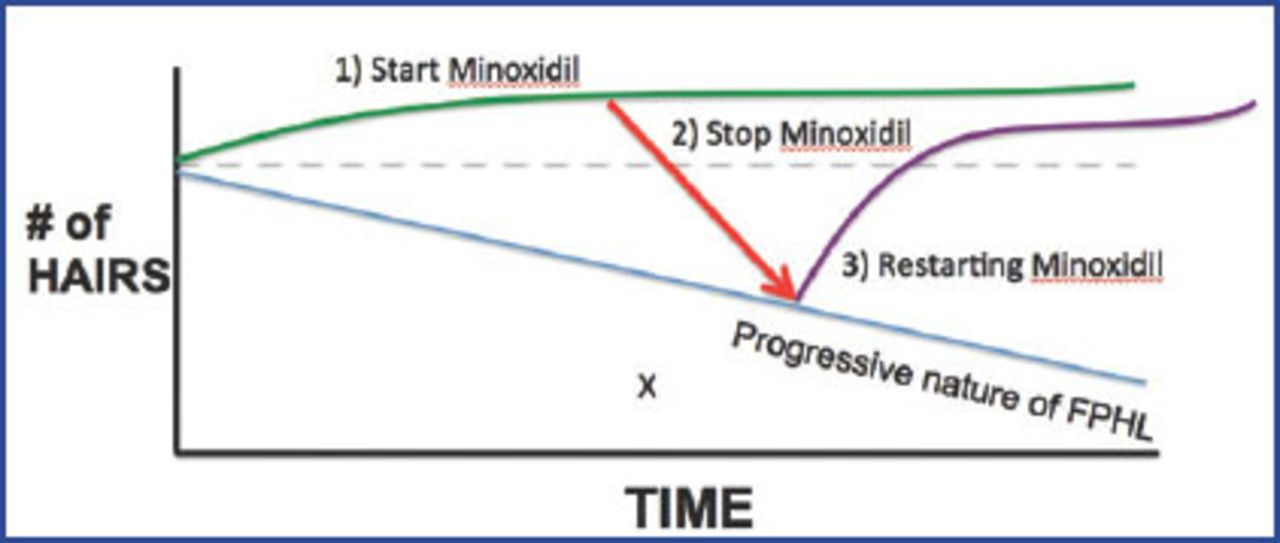
Perhaps the most difficult thing about getting women to use topical minoxidil is helping them to understand that it works. They often believe that because it is over the counter, it can’t possibly work. Or, they believe that if they stop it, ALL of their hair will fall out. Or that they have to use it forever. OR ELSE! These misconceptions can be addressed by drawing a simple diagram for your patients, using an x-y axis to demonstrate the natural progression of hair loss over time (Figure 2). By drawing a new (green) line, women can understand what will happen if they use medical therapy. And if they stop, they will just trend back to their natural course of thinning. By restarting, they will trend up again (purple line). They will not end up below this line (X), which is worse off than if they had never used the medication.

Minoxidil can still be a hard sell. Some women of Middle Eastern or Hispanic ancestry (or with polycystic ovary syndrome) may already suffer from significant hirsutism and do not want to worsen it with topical minoxidil. Other women in their 50s or 60s do not wash their hair more often than once a week, and dislike the idea of putting a product on the scalp every day and then not washing it out until they return to the salon. These women can benefit from off-label options like birth control pills, spironolactone, or finasteride.
Spironolactone
Spironolactone is a diuretic with anti-androgen properties. It can be helpful to explain to women that they have both estrogens (girl hormones) and androgens (boy hormones), and that in most women with FPHL these levels are NORMAL.7 However, their follicles are genetically more sensitive to circulating levels of androgens, specifically in the frontal 1/3-2/3 of the scalp (or on the sides). Thus, spironolactone helps to block these androgen receptors and can help prevent the miniaturization process on the follicle.8,9 Figure 3 shows an excellent response to 100mg/day over a 6-month period. The patient was an otherwise healthy 19-year-old female with a strong family history of thinning (father balded in his 20s). The patient was also advised to use topical minoxidil but admitted to using it only intermittently (once weekly).

Spironolactone can be an excellent choice for women with polycystic ovary syndrome, who already have signs of hirsutism or acne. The anti-androgen effects of spironolactone are already used widely in the field of dermatology to successfully treat both conditions. Women who are already on HCTZ or another diuretic for hypertension/fluid retention may be switched to spironolactone as a single agent to treat both conditions. This should obviously be done with the involvement of their internist. With rising health care costs, and an already complex health care system, such women are usually grateful for a drug that addresses two or more conditions. The data supporting the link between hair thinning and heart disease might imply that we should place all our FPHL patients on spironolactone!10
In order to slow down early thinning, patients may start at doses of 100mg/day. In order to achieve regrowth, higher doses of 200mg/day are generally required.11 The drug is a potassium-sparing aldosterone antagonist, so patients should avoid additional potassium supplements and make sure not to consume a lot of bananas. It also can potentiate sodium wasting (syndrome of inappropriate antidiuretic hormone, SIADH) secondary to selective serotonin re-uptake inhibitors (SSRIs). This should be discussed if patients are already on a drug such as fluoxetine or paroxetine. They can either take the full dose at once or spread it out over the course of the day (100mg twice a day). Their preference will generally be affected by whether the diuretic effect wakes them up at night. These patients may prefer to take it all as a single morning dose.
Other side effects can include breast tenderness, mid-cycle spotting, a diminution or disappearance of the menses altogether, or light-headedness. These can be reasons to gradually escalate the dose over a 4-6 week period. The author frequently writes for 50mg daily × 2 weeks, 100mg daily × 2 weeks, and 150mg daily × 2 weeks, and then has the patient come back to check potassium and sodium. If all is within normal limits and the patient is tolerating the drug well, their dosage may be upped to 200mg daily. Electrolytes should be checked every 3-6 months, increasing to every 12 months the longer the patient stays on the drug.
Due to the anti-androgen effect, women should not get pregnant on this drug. It is helpful to explain that the same anti-androgen effect that this has on the hair follicle it may also have on a male fetus. The author does not require all patients to be on birth control pills, but advises them to stop it immediately if they get pregnant.
Finasteride
Early data investigating the use of 1mg daily finasteride in women failed to show any improvement over placebo.12 One of the study’s authors (VP) suggests that this was likely due to the inclusion of women with senescent alopecia, which may not respond to any drug therapy. Subsequently, other studies done in the United States and around the world using higher daily doses of 2.5-5mg finasteride showed some significant results.13-15 The largest of these came from South Korea, showing that 70/86 (81.4%) of normoandrogenic women treated with 5mg finasteride for 12 months had improvement in global photographs. There were statistically significant improvements in hair caliber and hair density using scalp tattooing with microscopic scalp analysis.16
Widespread implementation for FPHL has been limited by concerns about breast changes or breast cancer. In the Propecia® post-marketing reports, there were reports of breast tenderness and enlargement in men. However, new data published in the Journal of Urology showed no statistically significant connection between breast cancer and the use of 5-alpha reductase inhibitors.17 Although this study was limited to men, it can make us more comfortable prescribing the drug in women. Recommending annual mammograms can help protect us as prescribers. Women with a strong personal or family history of breast cancer may still choose not to use this drug. Ultimately, the decision should be made by the patient and physician together. In the author’s experience, women are seldom put off by this potential risk and are grateful for another treatment option. Figure 4 demonstrates results before and 6 months after daily use of 5mg finasteride.

Finasteride can be a good alternative for women who have no cardiovascular risk factors (hence would not need spironolactone) or who already have a very complicated medical history (and you don’t want to interfere with their drug regimen). The physician should explain that it is metabolized by the liver but that there are no real drug interactions. It should only be offered to women who are not able to or are planning to conceive in the near future. These women should have undergone a hysterectomy, had their tubes tied, or be on 1-2 forms of long-term and reliable birth control. They must stop the drug IMMEDIATELY if they get pregnant. They also should not donate blood while they are taking the drug.
The medical literature supports the use of 2.5-5mg daily for FPHL. In the author’s experience, most women report no side effects. Insurance coverage varies: first, because it is approved for prostate enlargement in MEN, not WOMEN, and second, because insurance may consider hair loss cosmetic. Patients with access to Walmart may find finasteride on the “$9 list” for a 30-day supply of 5mg pills. Ninety days will cost them $24. Men taking finasteride may also benefit from this discount.
Dutasteride
Dutasteride blocks both type II and type I 5-alpha reductase enzyme, decreasing the levels of serum DHT by 90% versus 70% with finasteride. It has been successfully proven to help treat MPHL, but its widespread implementation has been limited by concerns about a long-term reduction in sperm counts. There is evidence that it can be very helpful in addressing FPHL, however, it tends to be more expensive than finasteride and we have fewer studies in women.18
Birth Control Pills and Other Anti-Androgens
Certain birth control pills may benefit women with hair loss. In particular, the brands Yaz® and Yasmin® (which contain both estradiol and drospirenone) appear to have the most efficacy. Drospirenone is a cousin to spironolactone, and can exert similar anti-androgen effects. Diane 35 is a birth control pill available in Canada containing cyproterone acetate. This ingredient is not US FDA approved. Although there is evidence that cyproterone acetate and flutamide, another systemic anti-androgen used to treat prostate cancer, can improve FPHL, their widespread implementation is limited by concerns about hepatotoxicity.19
Ketoconazole Shampoo
Given the observation that an inflammatory infiltrate rich in lymphocytes has been seen in areas of hair loss or balding, and that exacerbations of AGA have been seen with seborrheic dermatitis, a study was done to see if 2% ketoconazole shampoo could exert an effect on the thinning process. After 6 months in this small trial (39 patients total), the ketoconazole group demonstrated 18% improvement in hair density versus 11% improvement in the minoxidil + non-medicated shampoo group.20 It is still unclear whether the hair growth effect is through anti-inflammatory, anti-fungal, or anti-androgen mechanisms. Larger controlled studies are needed. In the meantime, it is an easy addition to the medical therapy since most patients have to shampoo anyway.
Topical Estrone Cream
There was a report in Greece using topical estrogen cream applied to the scalp of women with FPHL. In a study of 75 post-menopausal females, it demonstrated improvement (via decreased telogen rate and/or increased anagen rate) in 60-65% of patients applying a lotion with estradiol valerate .03% over 12-24 weeks. The side effects included postmenopausal uterine bleeding in 2 patients and breast cancer in one patient.21 An important concern would be the development of an estrogen-dependent tumor, especially in a person with family history of breast or uterine cancer. Dr. Bobby Limmer reports recent use of this compound, and has been seeing quite impressive results. His data is forthcoming. In the meantime prescribers should balance the risks with the benefits for all possible patients.
Pregnancy and Lactation
If a patient is planning to get pregnant in the near future, she should not be prescribed either spironolactone or finasteride, given the risk of birth defects. Patients can continue with topical minoxidil right up until they get pregnant; however, they should stop when they get pregnant because there are isolated reports of birth defects. Patients can be reassured that the hair will thicken during the course of their pregnancy. The hairs will enter a resting telogen phase and won’t shed until 3-6 months after the baby is delivered.
Patient Satisfaction
Although it can be time-consuming, patient photography is essential to motivating patients. The author takes standard photos at the initial visit, with the hair parted down the middle and pinned to the sides. The chin should be turned slightly down so that the anterior and posterior aspects of the part are equidistant from the camera lens. Similar lighting, backdrop, and distance to camera are ideal. Patients should return for follow-up at 6-12 month intervals to assess their results. The author uses an iPad with photos uploaded from their previous visit. Many patients think there is no improvement until they see their old images and cannot believe their eyes!
Hair Thickening vs. Hair Growth Products
There are a large number of products on the market that claim to “instantly increase density” of hair. Such products are usually in the form of shampoos, conditioners, or serums applied to the hair. These products can be very effective at coating the hair shaft so that it feels thicker. However, the results will only last until the next hair washing. Patients should understand the difference between these products and those that actually can make the hair GROW thicker!
Conclusion
While the medical treatment of FPHL can be challenging, it can also be extremely rewarding. Patients are relieved to know they have options, and thrilled when they see results. In advanced cases, this may require some trial and error, or a combination of therapies (Figure 5). Successful treatment of young women can be especially satisfying because we are improving their sense of confidence for a lifetime ahead.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Editor’s Note: We are indebted to Dr. Nicole Rogers and to Dr. Bernard Nusbaum (see Editor Emeritus) for their articles on female pattern hair loss (FPHL) in this issue of the Forum. They bring the current thinking on the medical treatment of this difficult condition into focus. Hair transplantation is often also available for these patients, but it’s more difficult than in males and would make a suitable subject for another time. While we can currently make some difference for female hair loss sufferers, most of us working in this field would be happier if we could do more. We hope that something better will come along and soon. Already there are many doctors using PRP in hair loss but scientific studies are few. Anecdotally, the reports, however, are encouraging.
As in so many difficult to treat conditions there is an inverse relationship between the number of therapies and the likelihood that any will be of great benefit. Thus, the plethora of treatments for FPHL, noted our esteemed colleague, Dr. Bob Haber, in a recent communication.
Understanding the pathogenesis of FPHL is the first step, then therapy should be made easier. We are getting closer but not there yet. —MM
- Copyright © 2014 by The International Society of Hair Restoration Surgery
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.
- 9.
- 10.
- 11.
- 12.
- 13.
- 14.
- 15.
- 16.
- 17.
- 18.
- 19.
- 20.
- 21.