
Most of us would agree FUE harvesting is generally a more labor intensive manner of harvesting when compared with traditional strip excision harvest. Also, transection rates tend to be higher when compared with strip harvest in selected cases. Below, Dr. T.K. Shiao shares with us an innovative design for improving graft harvest quality in FUE donor cases. His design is unique in that it takes into account ergonomics as it relates to the functional anatomy of the wrist.
Sharing our ideas makes us clinically stronger as a collective group in the ISHRS. Please feel free to email me your ideas at tcarmanmd{at}mac.com for consideration for publication in our journal.

Introduction
Since Drs. William R. Rassman and Robert M. Bernstein first described FUE in the medical literature in 2002, the innovative efforts of Dr. James Harris (S.A.F.E.), Dr. John Cole (F.I.T.), Dr. Robert True (Osada), and many others have improved upon the techniques and technologies related to FUE. In doing so, this has created a potential rival, in terms of outcome results, for FUT.
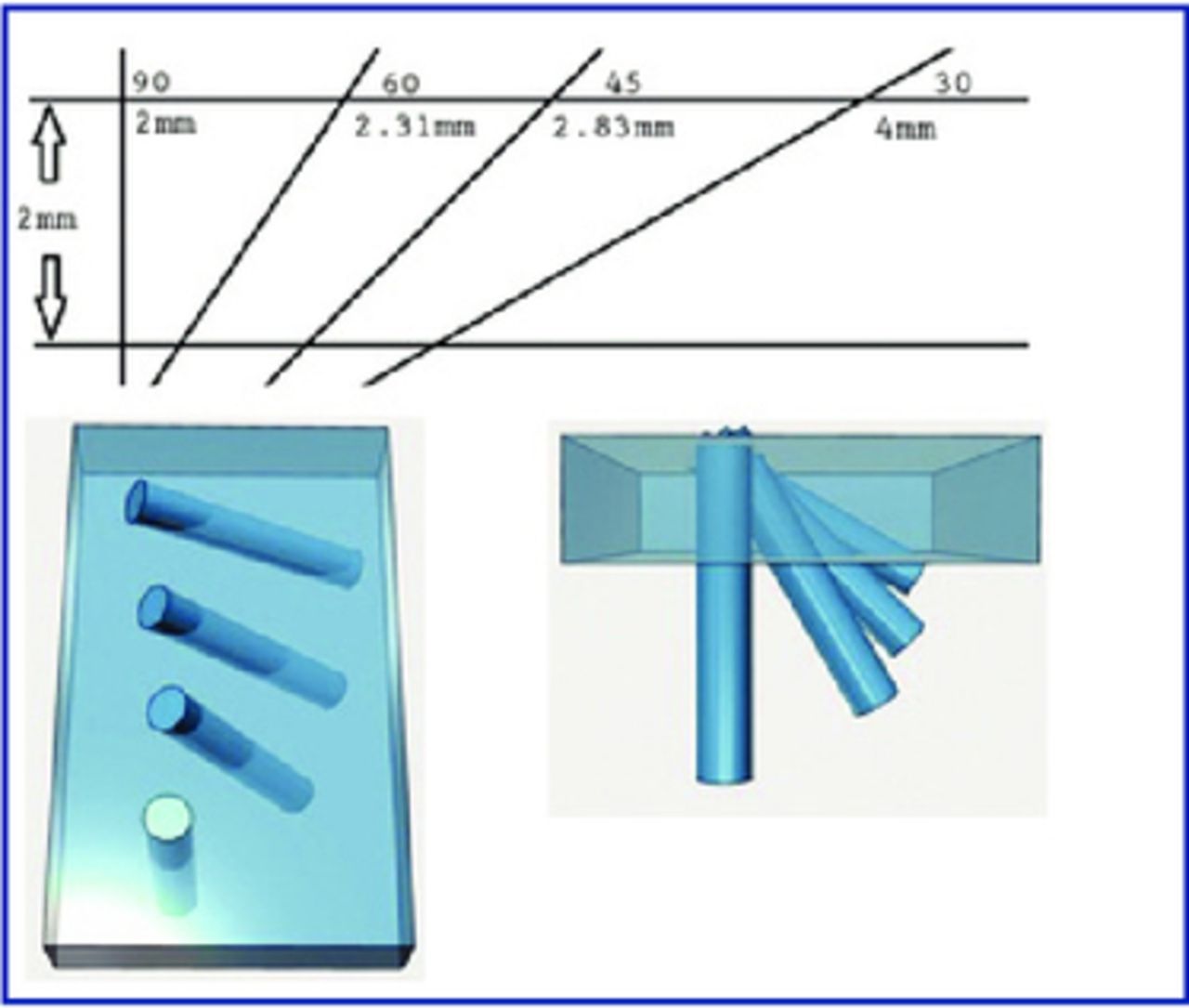
Harvesting good grafts with FUE, however, remains a daunting task for the inexperienced. And even in experienced hands, situations that require deeper penetration, such as long follicles, thicker dermis, or acute exit angles, may still result in higher than normal transection rates. Figure 1 shows how different exit angles influence the necessary distance required to punch through the same thickness of dermis.
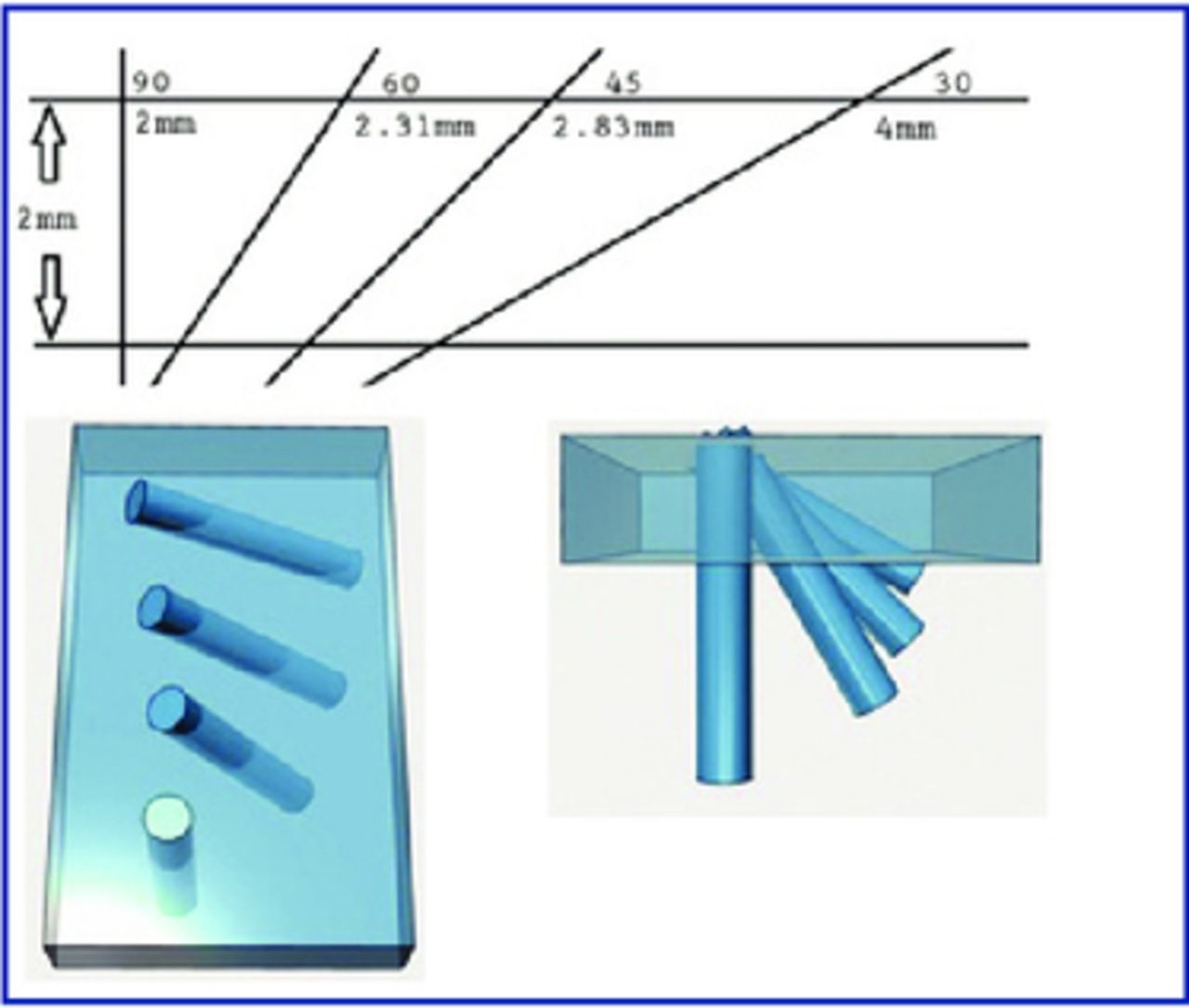
Simple trigonometry shows that even a small change in exit angle can greatly increase the distance a punch must travel in order to penetrate the same 2mm-thick dermis; note the significant (73%) increase between 60 degrees (2.31mm) and 30 degrees (4mm).
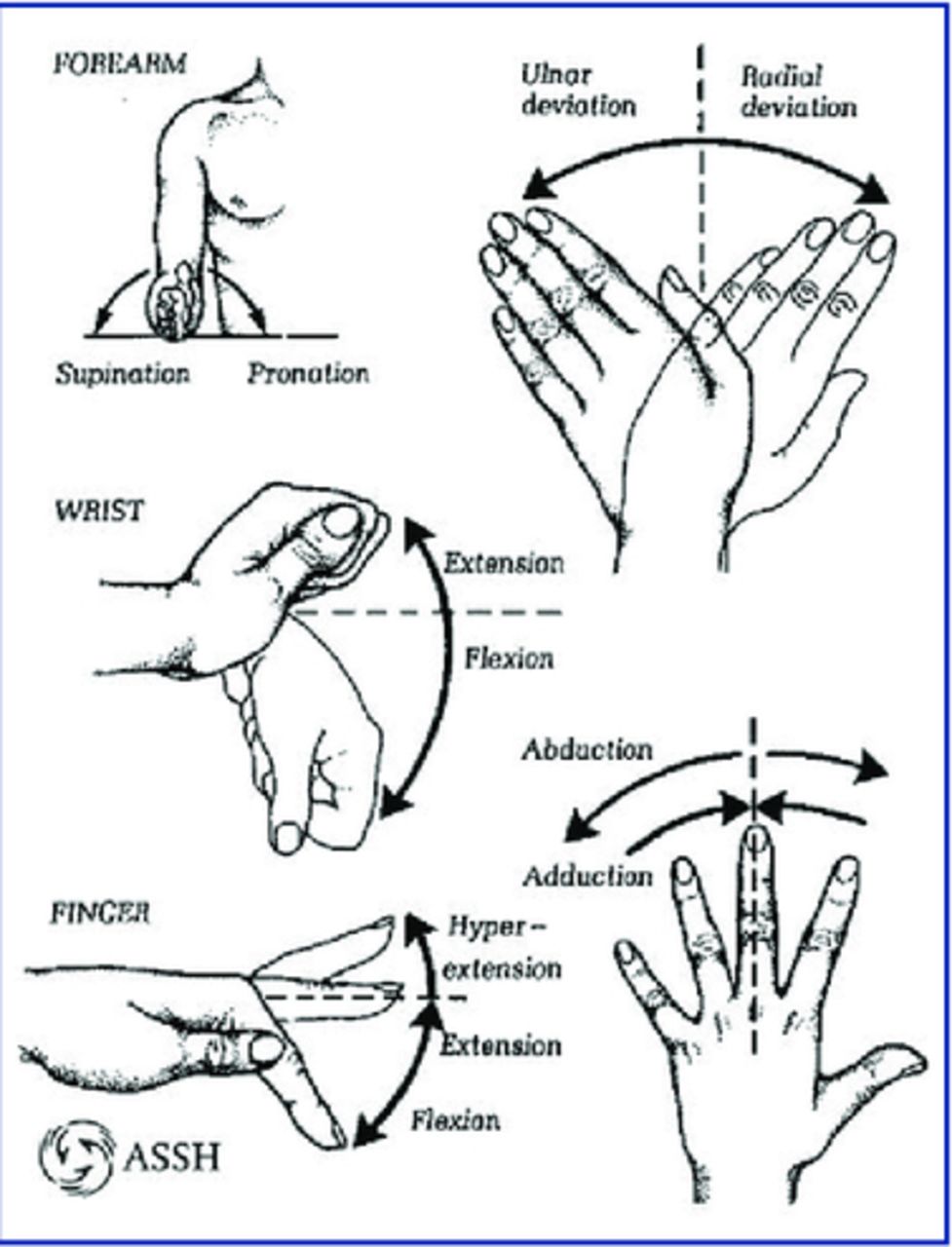
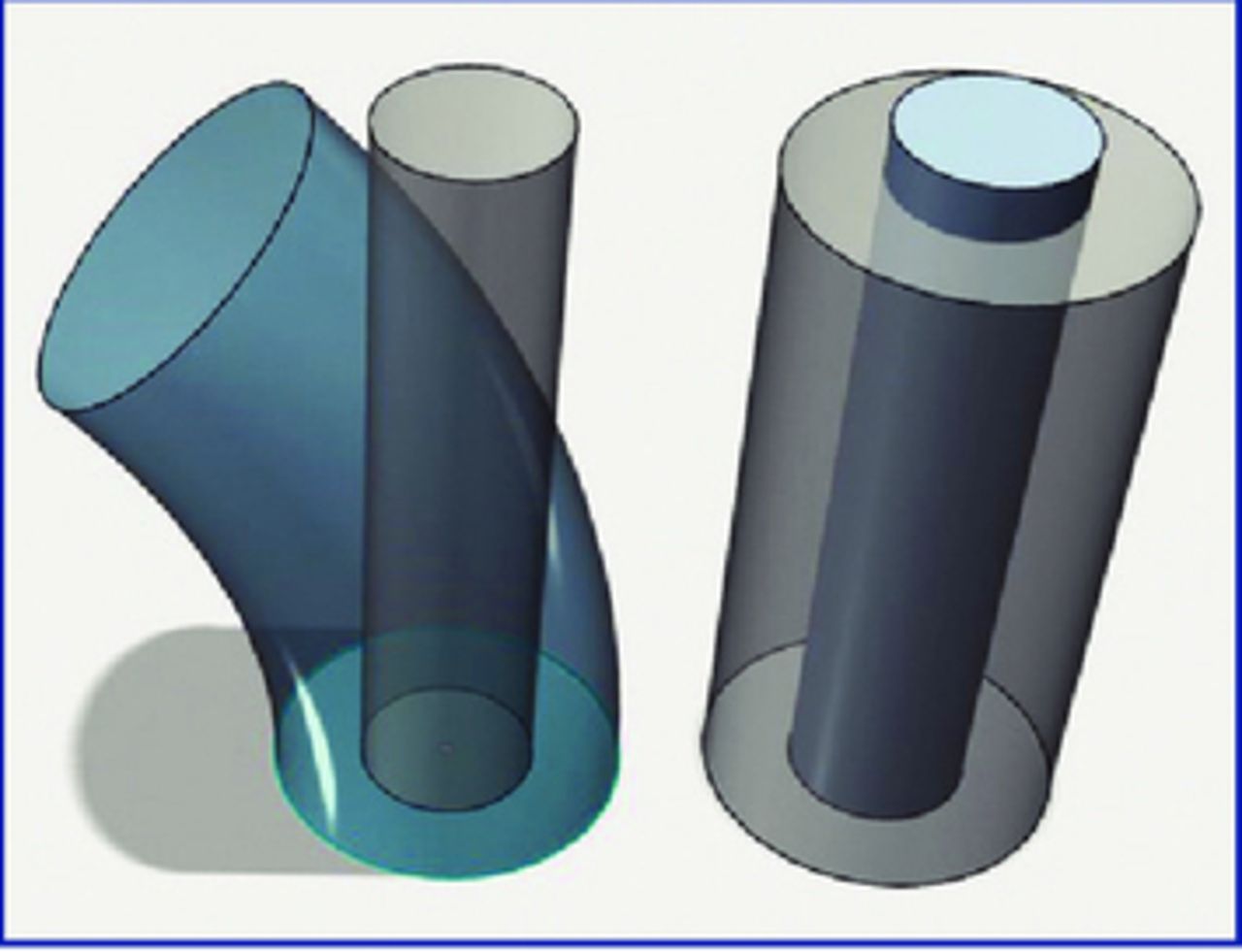
While the causes of follicular transection are multifactorial, the inability to advance a rotating punch in a true linear fashion likely plays a significant role. First consider functional anatomy. Articulating at the wrist, the hand naturally swings in an arc (Figure 2). The traditional rotating FUE punch produces a 2-dimensional cutting circle. Combining this cutting circle with a long arc increases the chance of the cutting surface intersecting the follicular unit, causing partial to complete transection of the follicular structure (Figure 3). To advance the punch following a true linear path, however, requires compensatory movement in other parts of the upper extremity. This can contribute significantly to increases in muscle tension and fatigue.

Wrist joint movements. Reprinted from Essentials of Hand Surgery.

Arced Path (left) vs. Linear Path (right). Smaller cylinders inside represent follicular units; outer surfaces represent the cuts made by arced vs. straight cutting path.
Description
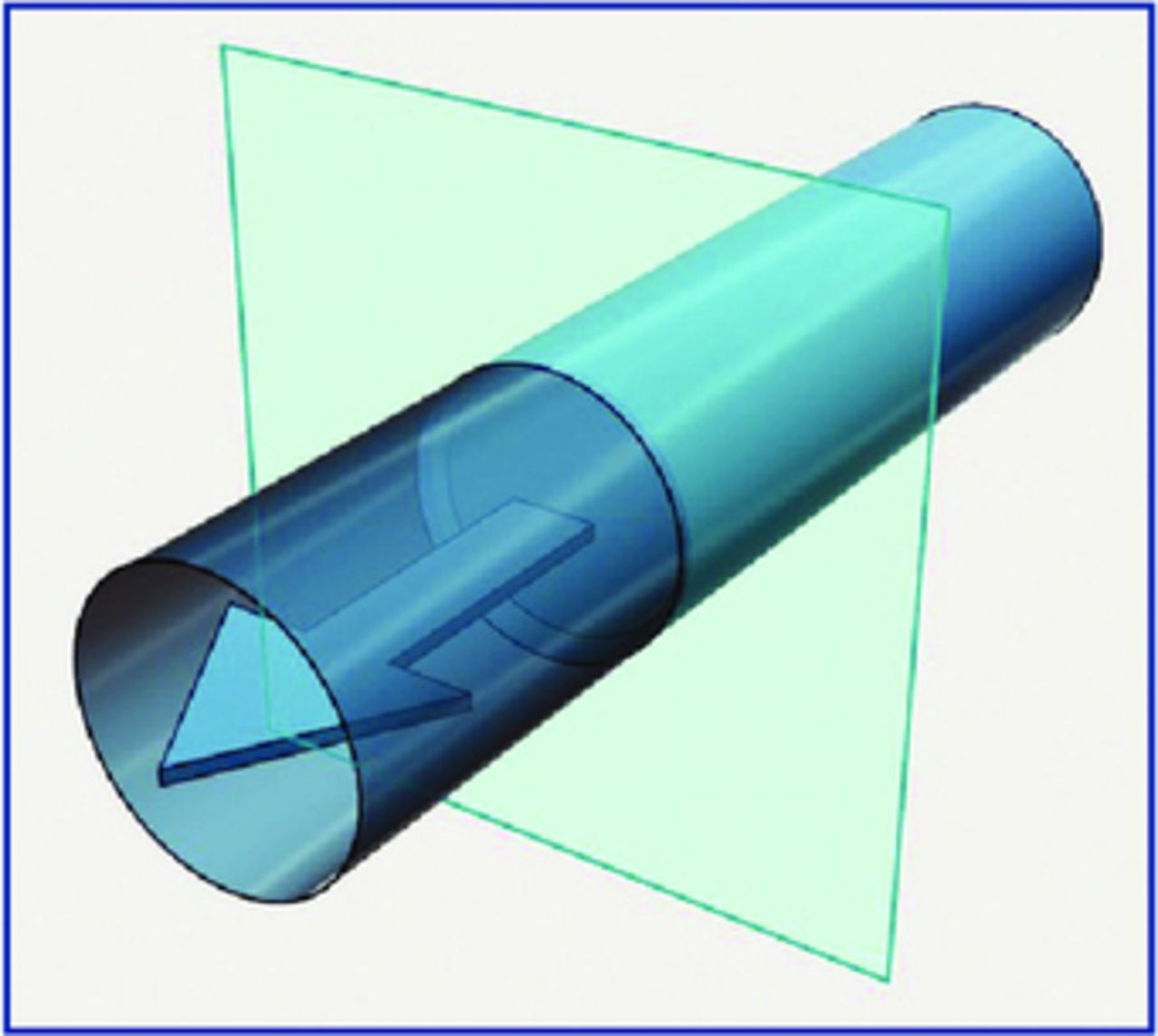
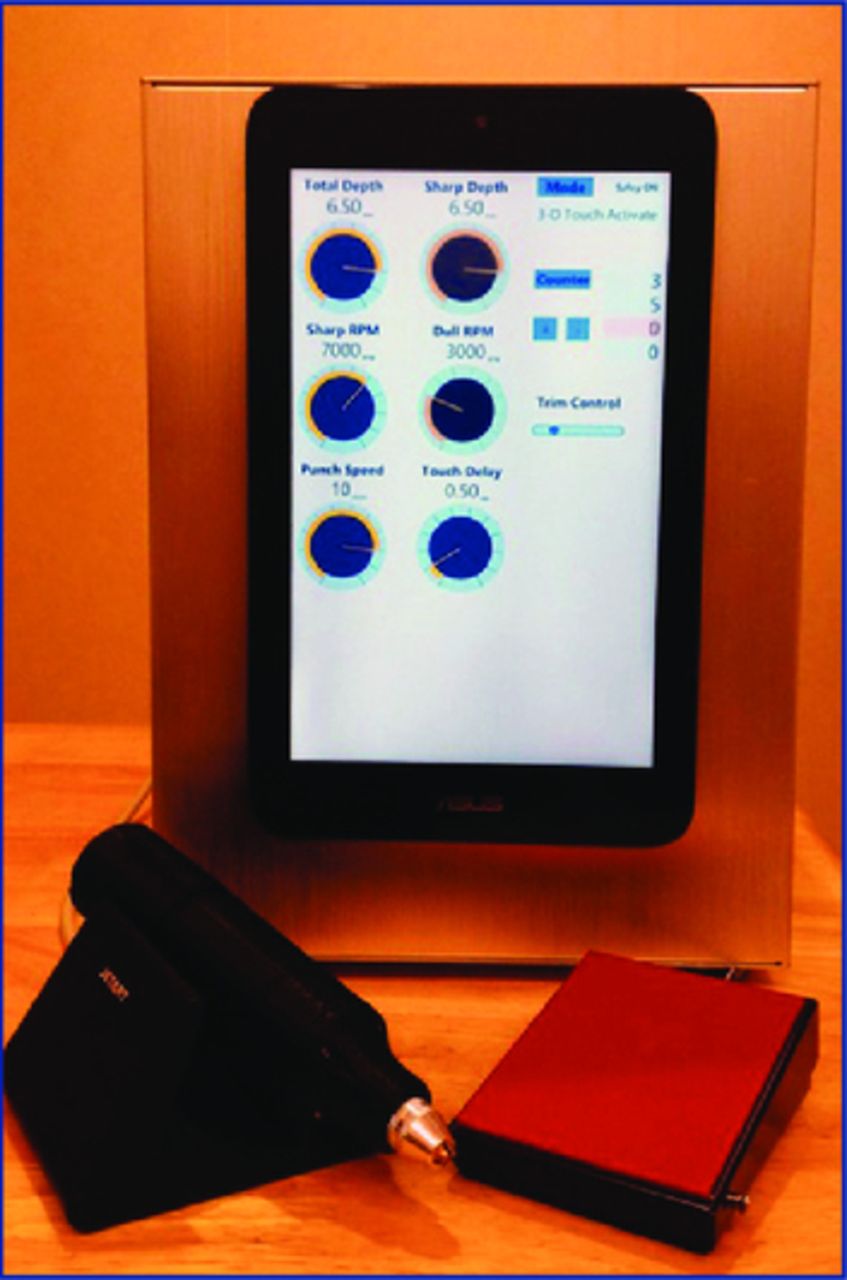
3D FUE minimizes the aforementioned difficulty by adding a third dimension to the traditional rotary punch. By creating a special handpiece that moves the cutting circle in the axial direction, it creates a 3D cutting cylinder (Figure 4). Figures 5 and 6 show how the chuck and punch move forward during the process. A microprocessor controls the rotation and the advancement, allowing tremendous flexibility in the design of the cutting action. Figure 7 shows the control unit of the 3D FUE system. Touch activation of the 3D cutting process further simplifies the operation. The surgeon simply lines up the punch with the direction of the hair follicle, touches the scalp with the punch, and allows the machine work. Furthermore, when the safety foot switch and the touch activation are fully utilized, the operator can precisely position a non-rotating punch over a hair follicle before 3D cutting commences, further lowering the learning curve.
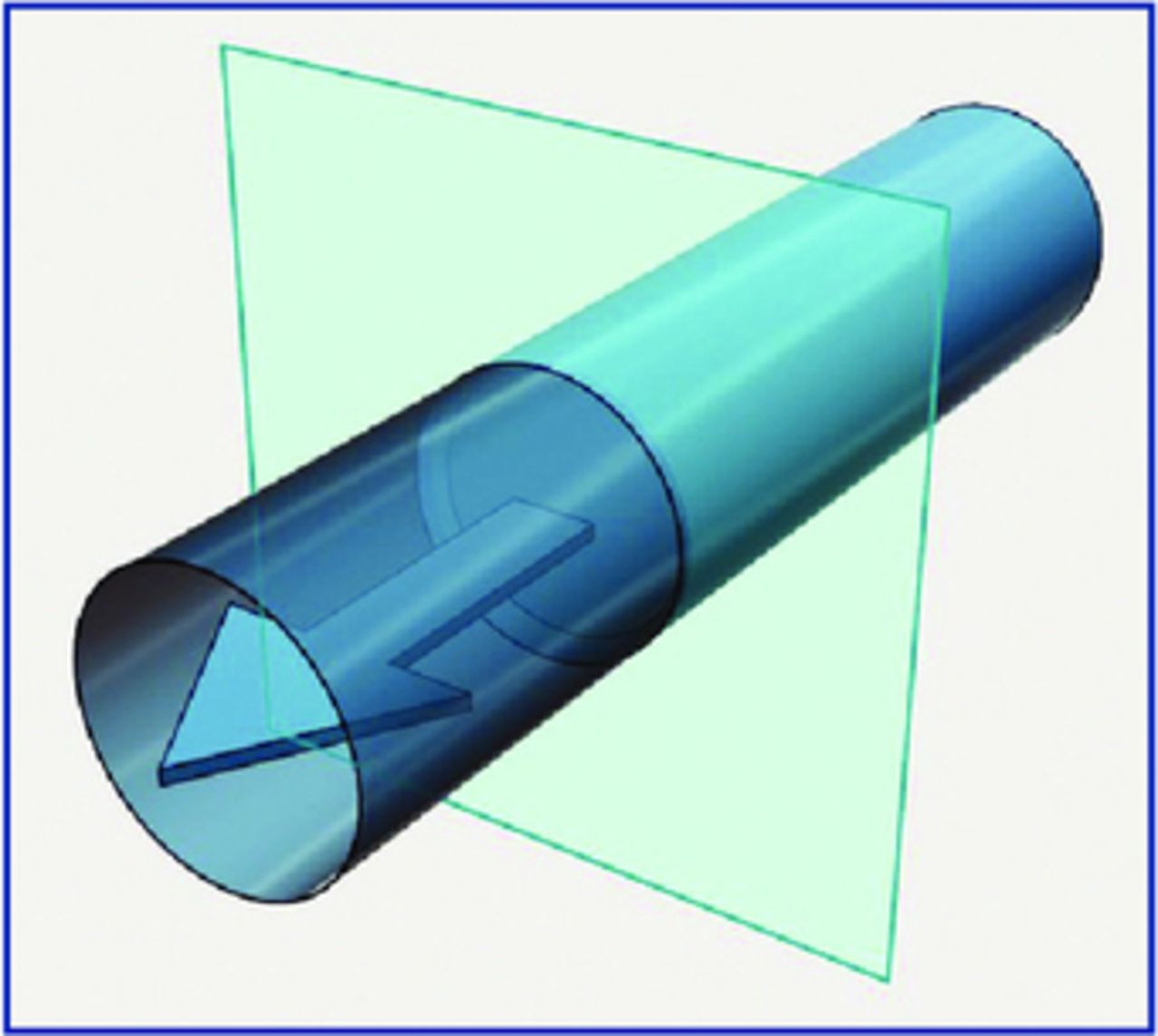
3D FUE adds a new dimension along the axial pathway of the 2D circle cut by traditional FUE motors. As the motor/assembly turns and advances, a perfect 3D cylinder is cut.

Touching the scalp activates the rotation and the advancement of the punch.
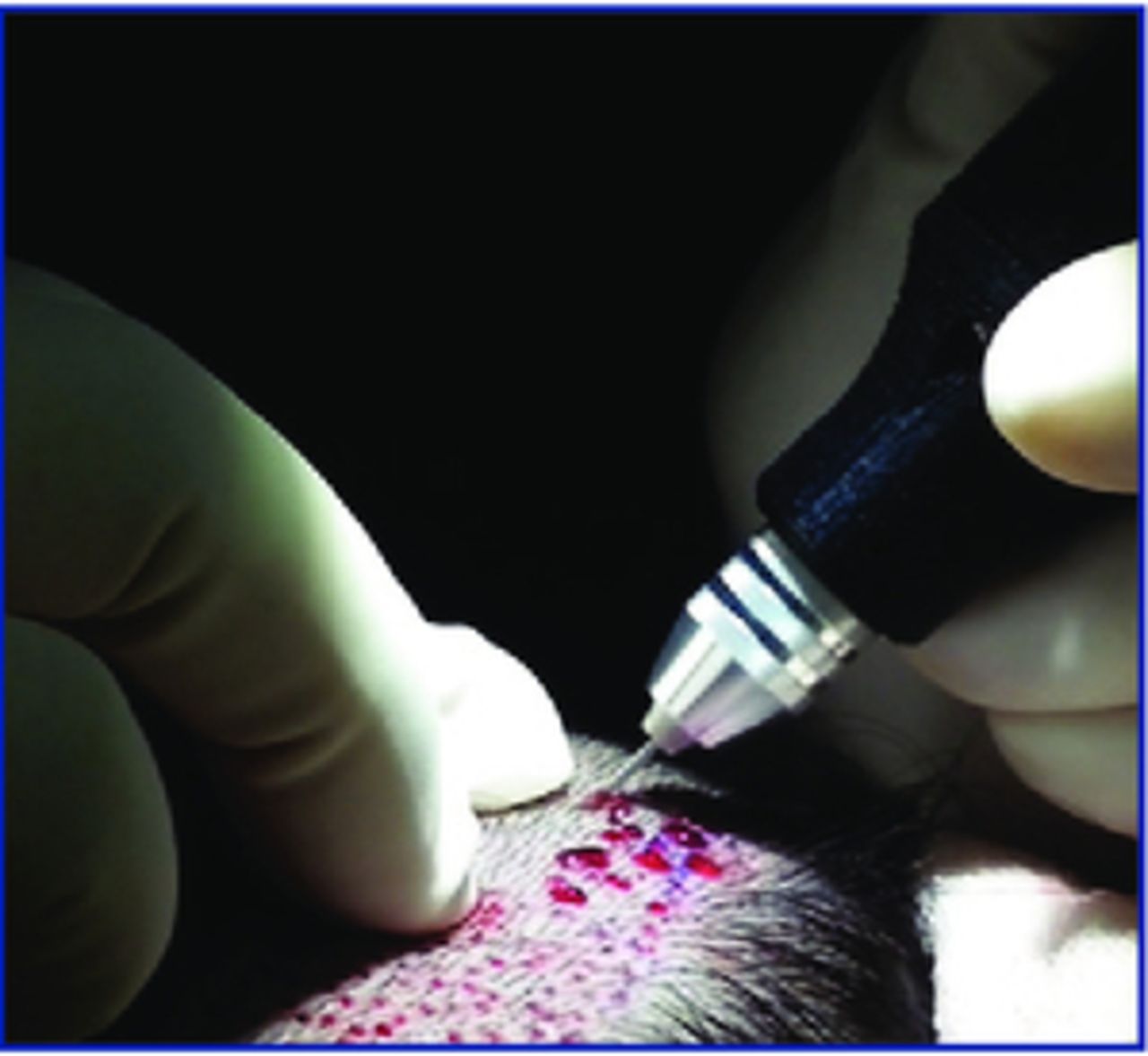
The punch is advanced to the depth set by the operator.
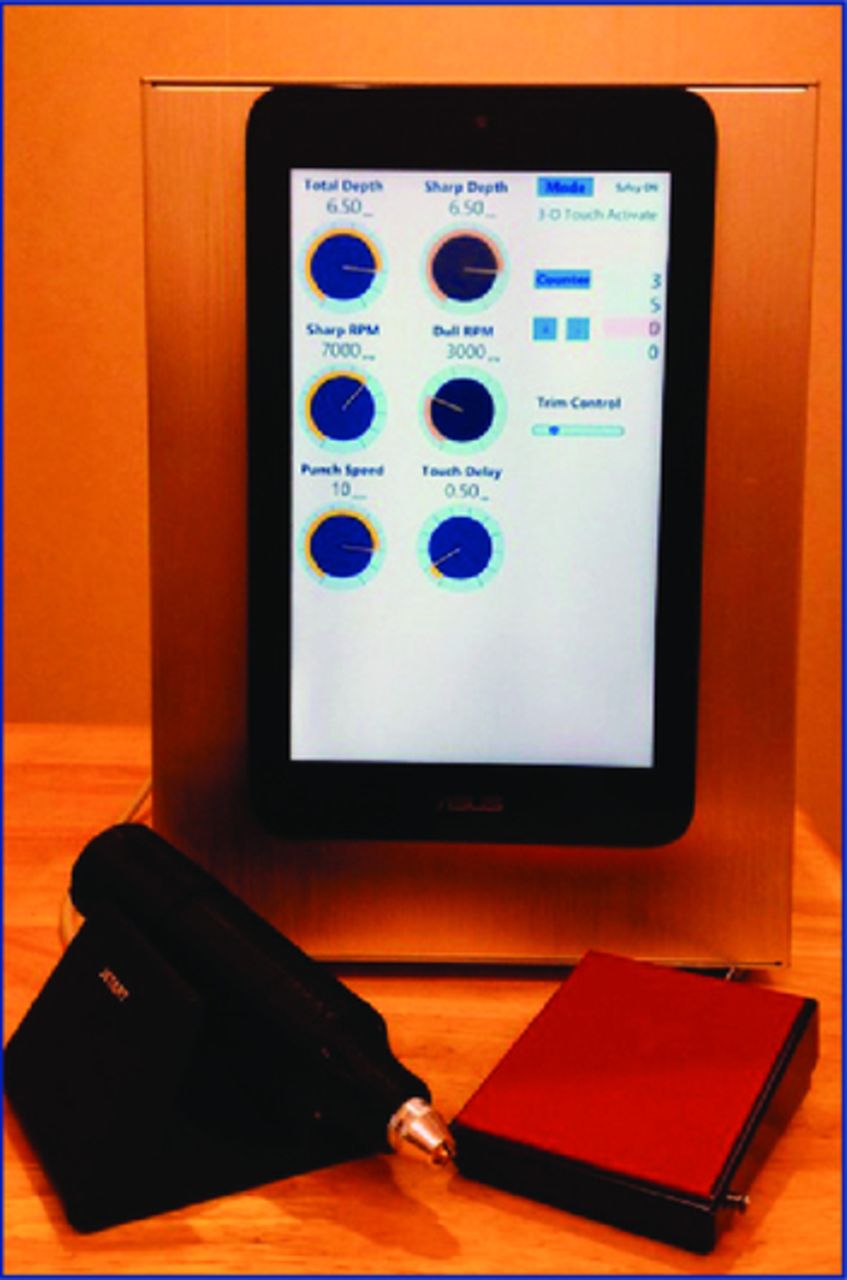
The control unit shows how flexible the system is.

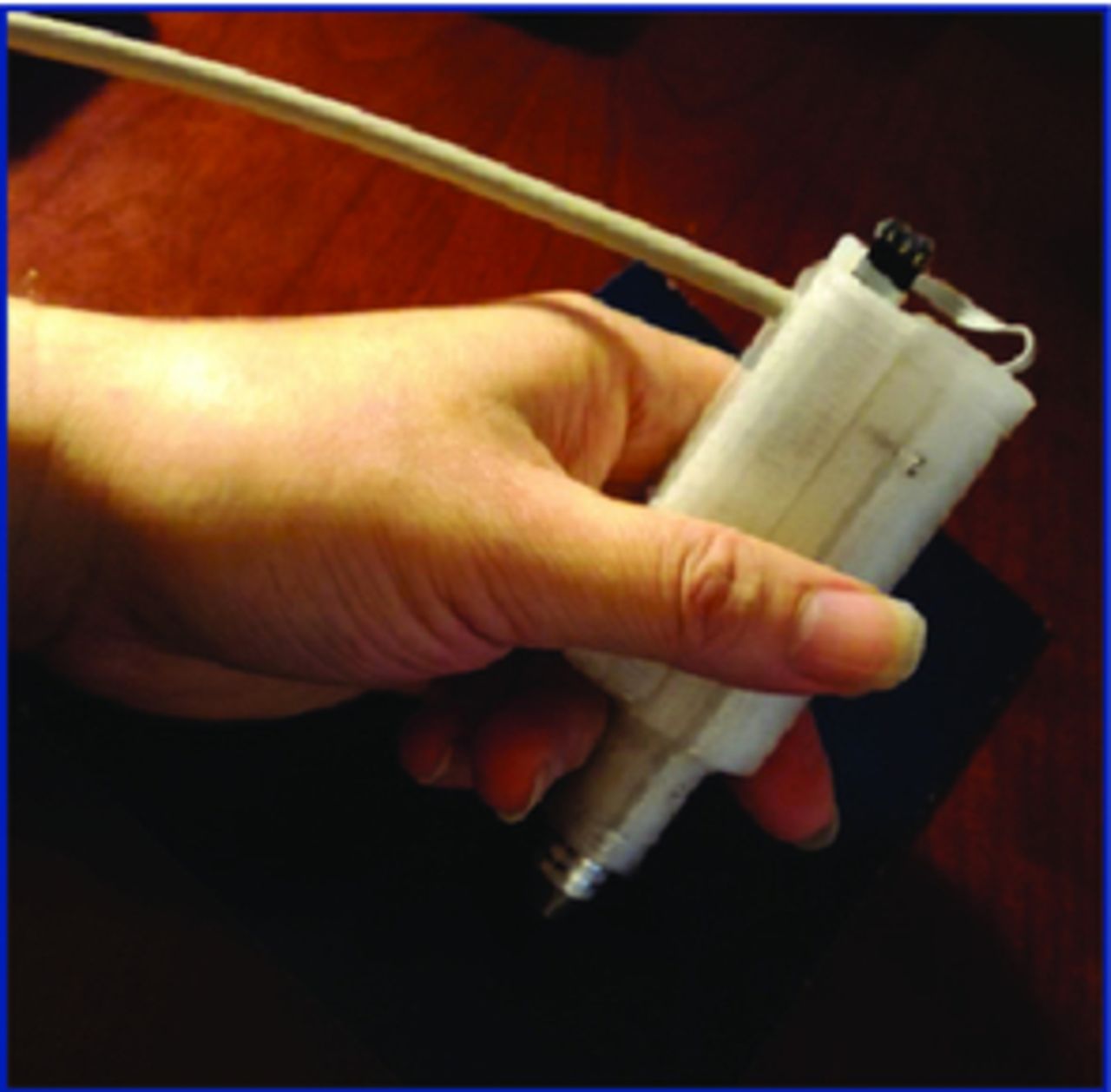
Standard orientation handpiece.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
“Shorty” for maximum maneuverability.
The following are advantages of 3D over traditional 2D rotary punch:
There is a true linear path of punch advancement; this is particularly beneficial for long straight hair follicles, thick dermis, and hair with acute exit angle.
There is precise linear movement, which may also allow for a smaller punch.
It allows for active depth control versus the passive depth control found on the 2D rotary punch.
The punch does not start rotating until it touches the scalp, making the handpiece safer to handle.
It has a versatile chuck that accepts most existing punches on the market.
It uses a long tubular punch, which provides better directional aim (rifle vs. handgun).
Its lightweight and short handpiece with side exit cable maximizes maneuverability.
It has a disposable handpiece, which makes it maintenance free.
The disadvantages of the 3D are limited to the following:
The initial investment makes it more expensive than the traditional 2D rotary punch, but it is significantly cheaper than a robot.
The disposable handpiece gives the appearance of higher cost per case. This cost can be easily offset by the reduction in transected follicles and the elimination of traditional handpiece maintenance costs.
Conclusion
Mechanizing the linear advancement of a rotating punch added a much needed third dimension to the power FUE device, particularly when deeper penetration is necessary to facilitate extraction. Eliminating a challenging manual skill necessary for FUE, 3D FUE lowers the learning curve for beginners. 3D FUE also increases the rate of harvest and decreases the rate of transection for those who do not perform FUE regularly. Mechanizing a repetitive action also reduces repetitive motion injury and potentially reduces muscle tension for any operator, from the novice to the advanced.
Punch movement activation requires the safety foot switch to be depressed and for the punch to physically make contact with the scalp. This two layer activation sequence lowers the learning curve further by allowing the operator to precisely place a non-rotating, thus non-cutting, punch over the follicular unit of interest before commencing the 3D cutting process using the safety foot switch.
Lastly, in this author’s opinion, it is fun to use.
Footnotes
Disclosure: Ownership Interest, Patent and Patent Pending
- Copyright © 2016 by The International Society of Hair Restoration Surgery