
Grafts are different in FUE and FUT. In FUT, the grafts have tissue surrounding the entire length of the follicles. In FUE, the portion of the grafts near the bulbs often is stripped of tissue, which leaves them more vulnerable to both desiccation and trauma during removal, processing, and, most of all, insertion. Skilled hands can place grafts properly with forceps without damaging the follicles by grasping the tissue below and adjacent to them rather than the follicles themselves. In FUE, however, there is a greater chance of trauma and consequent poor growth with forceps because the follicles themselves are touched.1 Implanters promise to be the answer for this problem.
Implanters are not new. Choi published an article in 1992 presenting a new implanter device, designed to simultaneously make recipient incisions and place grafts without touching the follicle bulbs.2 Since then, implanters have become very popular in Asia, but are used by only a minority of surgeons elsewhere.3,4 Perhaps this has been true because patients of other ethnicities have finer hair of higher density or very curly hair. Another possible explanation for the lack of acceptance is that in many practices graft placement into premade sites is delegated to assistants, and sharp needle implantation requires the surgeon to place the grafts.
Because in FUE the surgeon harvests all the grafts, placing all of them with sharp implanters using stick-and-place can be exhausting and can limit the amount that can be accomplished in a single procedure. Another problem with implanters is the cost. Each implanter’s needle costs US$15.00 and 6-8 of them (three to four for single-hair grafts and the same number for 2- and 3-hair grafts) are usually required for each surgery. In case needles get dull, they must be changed during the procedure. In addition, implanters must be replaced regularly as they don’t last long when autoclaved.
Using dull needle implanters solves these problems (Figure 1). Recently, Dr. T.K. Shiao developed implanters to place grafts into premade sites.5 We have developed a similar system using regular implanters with dull steel needles. We will compare the advantages and disadvantages of this approach to premade sites forceps placement, and also to sharp implanters.
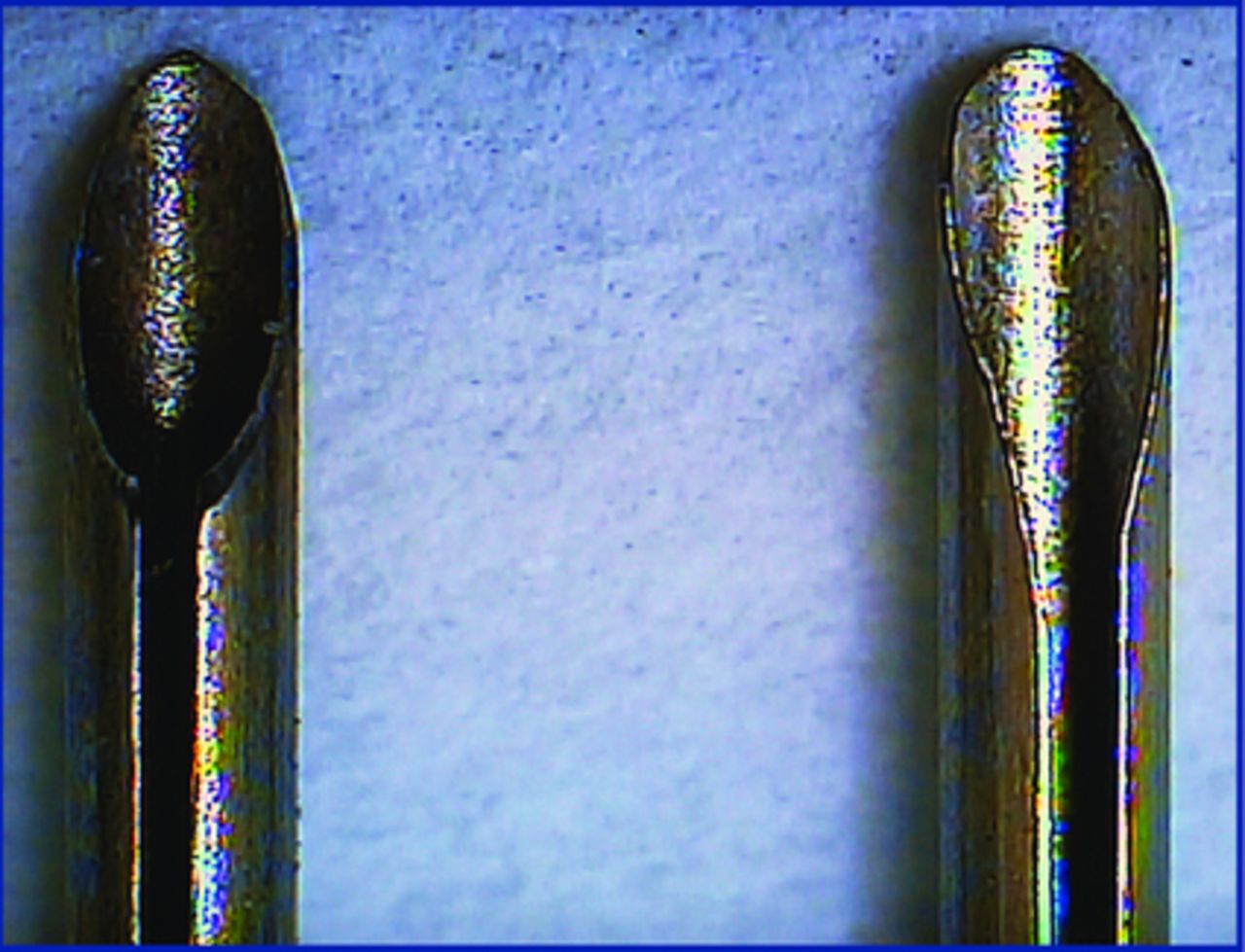
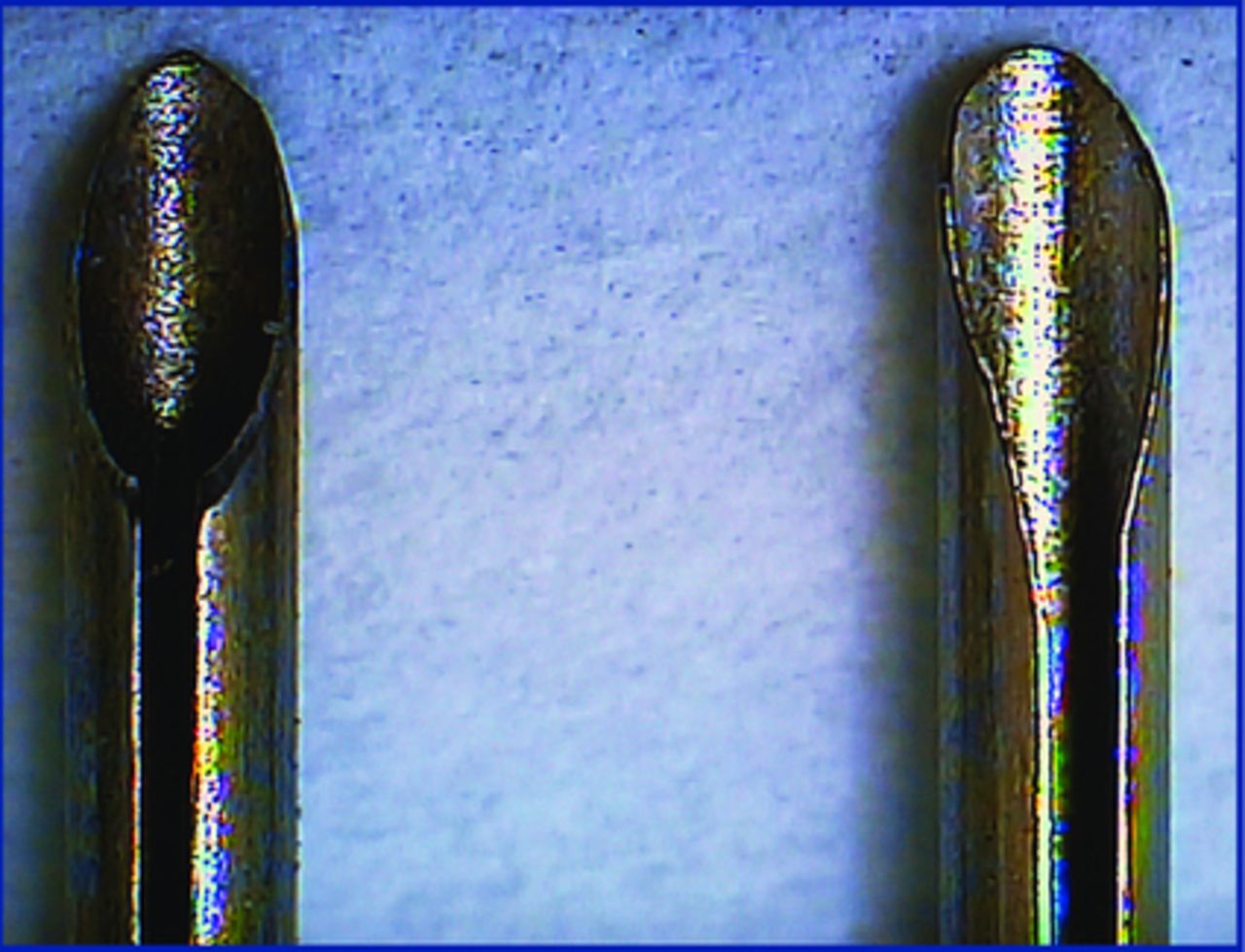
A sharp and modified dull KNU implanter needle
Main Advantages
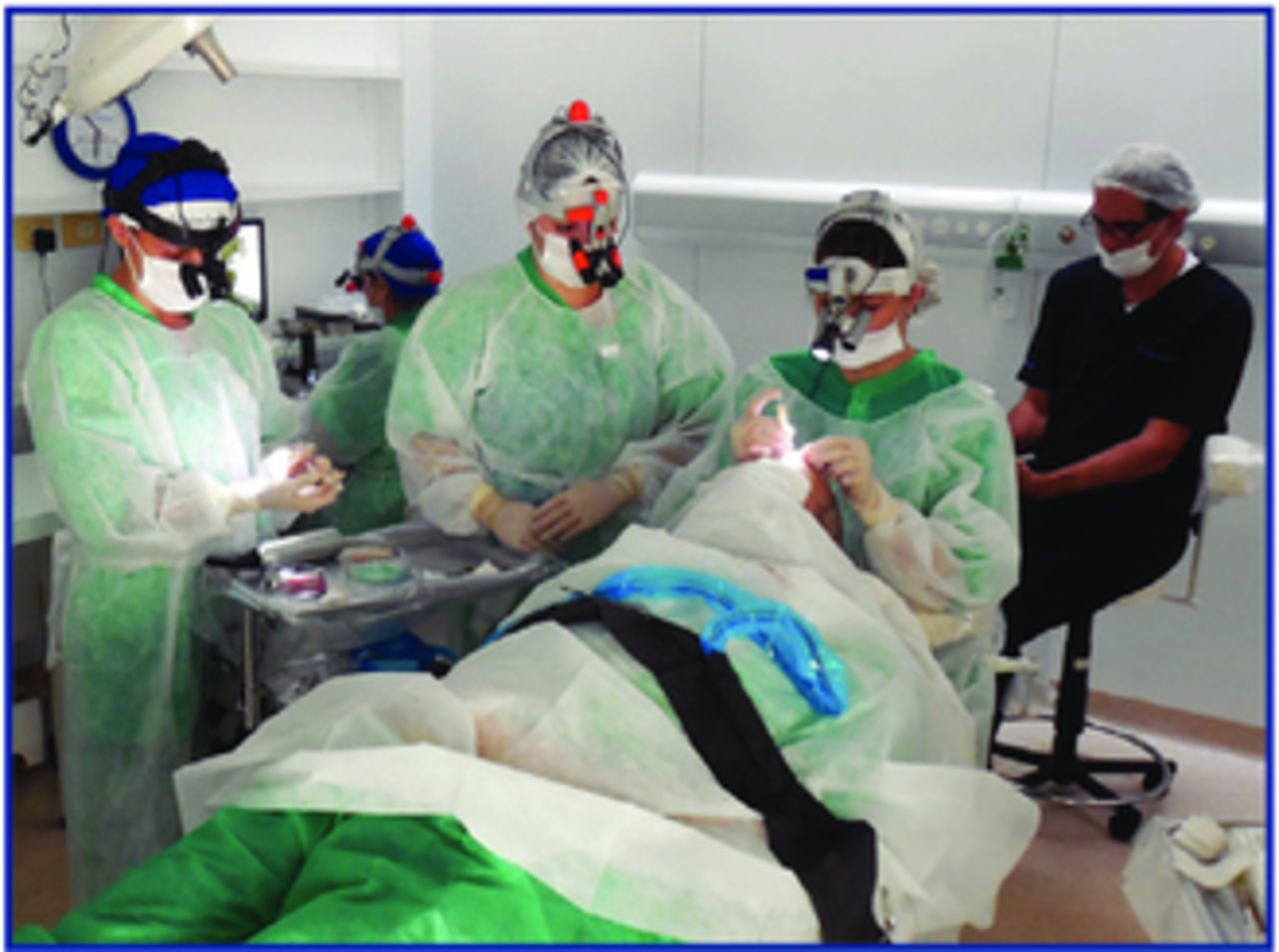
Delegation of work. Premade sites allow the surgeon to delegate the work of placement after graft harvesting. Surgical assistants, whether physicians or not, can place a few hundred grafts while the surgeon rests between harvesting sessions (Figure 2). In order to minimize time out of the body, and when harvesting and placement simultaneously is not possible, we routinely harvest from 300-400 grafts and place all of them before harvesting additional grafts. This optimizes yield and produces a comfortable cycle of activity and rest for both the surgeon and the staff. When we are harvesting with the patient lying on their side, harvesting and placement can occur simultaneously with the implanters (Figure 3).
Minimal trauma, optimal growth. Implanters allow placement without risk of follicle damage such as that which occurs when too much pressure is applied to the graft with forceps. Important in any technique, but essential in even more fragile FUE grafts (Figure 4).
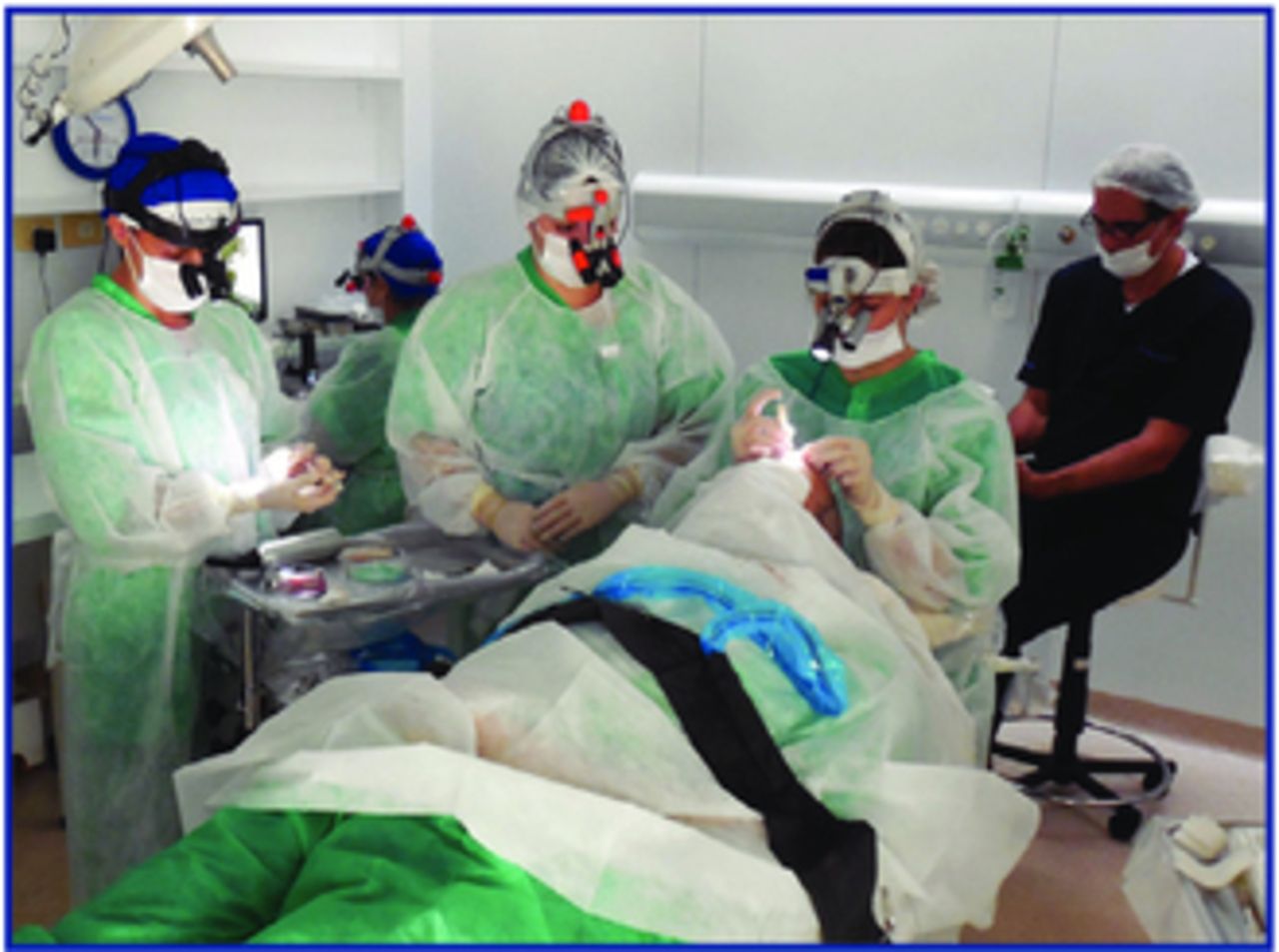
Surgeon resting while grafts are being placed.
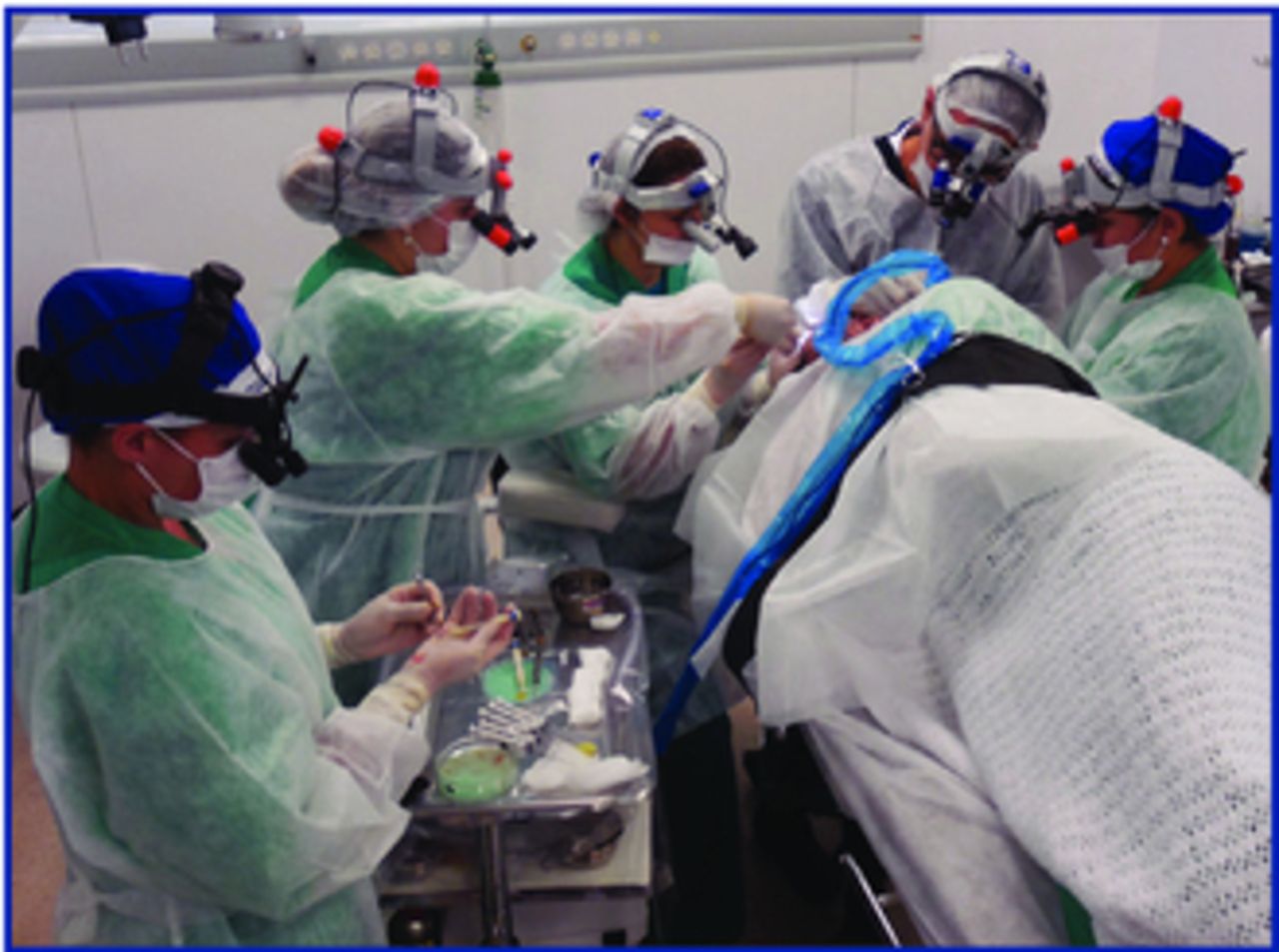
Grafts being extracted and placed simultaneously.
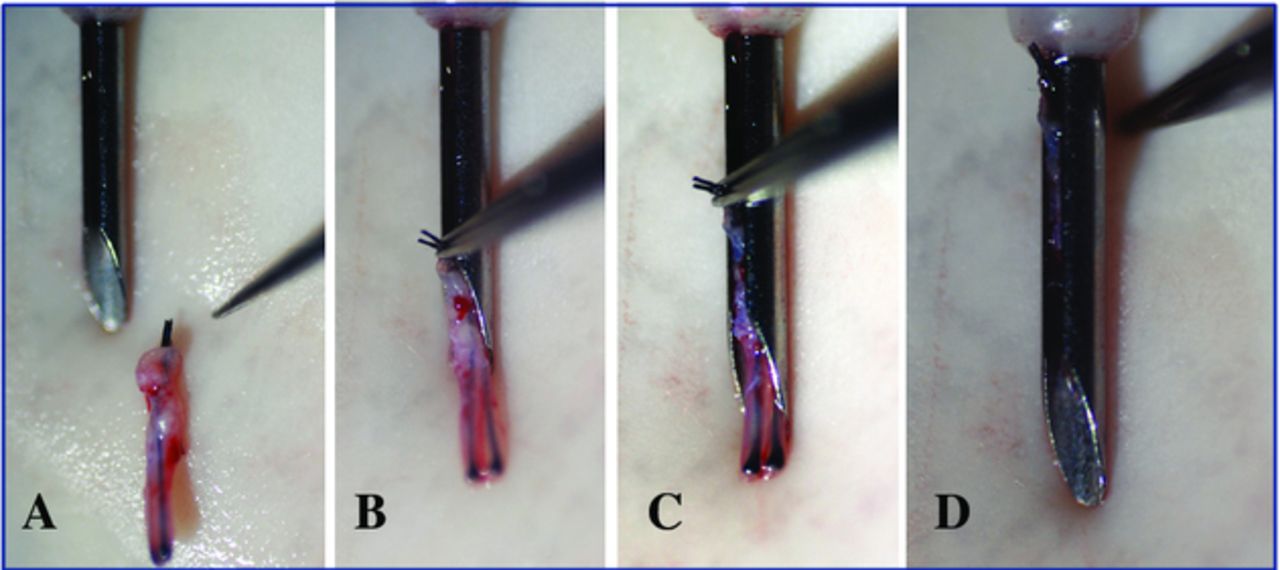
A-D: Dull needle implanter is loaded.
Secondary Advantages
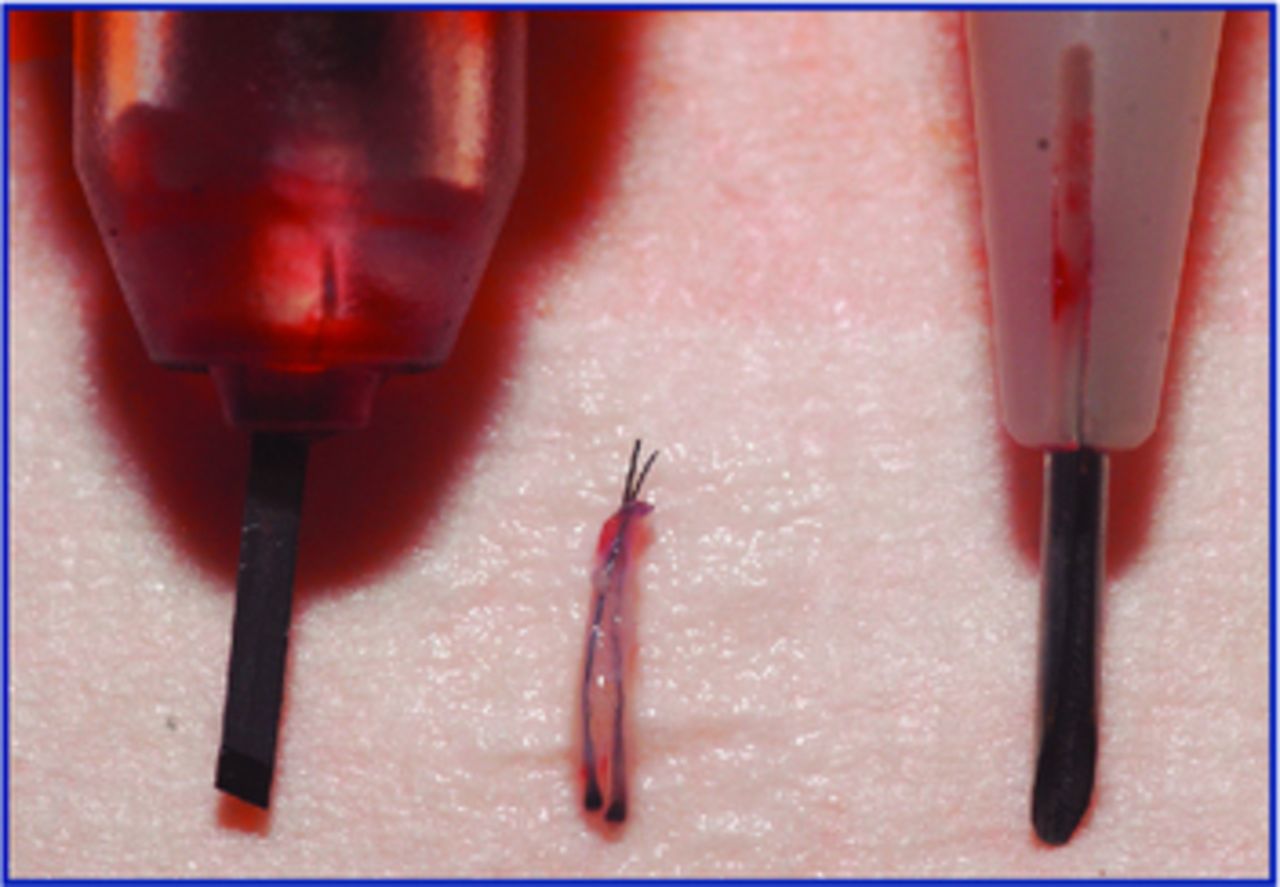
Smaller incisions. Usually, we harvest grafts with 0.9mm punches. Because the grafts contract a little, their final diameter is less than 0.9mm. With sharp needle implanters, the size of the recipient incisions is determined by the size of the needles (Lion®: 0.64mm and 0.8mm for singles and 1.00mm for 2- and 3-haired grafts. KNU®: 0.74mm and 0.82mm for singles and 0.96mm, 1.02mm, and 1.14mm for 2- and 3-haired grafts) (Figure 5). One of the most important advantages of the dull needle implanters is that the size of the premade recipient incisions can be much smaller. Smaller incisions allow higher densities and less trauma to the recipient area. For single-hair grafts, we make 0.63mm premade incisions (23g needle) and place the grafts with 0.74mm dull needles (Figure 6). For 2- to 3-haired grafts, we make 0.8mm to 0.85mm premade incisions and use 0.96mm dull needle implanters (Figure 7).
Shorter learning curve. A surgical assistant requires many months of training to place grafts with forceps.5 Training one to use implanters requires just a few days. This makes it easier to replace staff when the need arises.
Less expensive. Implanters with dull needles can be resterilized and used over and over again. We sand off the edge and point of regular needles. We prefer needles of steel without plastic hubs, which can be sterilized more effectively in a longer autoclave cycle. We have found modification of the KNU implanters rather than the Lion implanters preferable for this reason (Figure 8).
Harvest and place at the same time. With the patient lying on their side, the surgeon can harvest grafts while the assistant places with implanters.
More accurate. With premade sites, the angle and depth of incisions are better controlled, whereas with stick-and-place (with forceps or sharp needle implanters) there is more variability resulting in uneven final results.
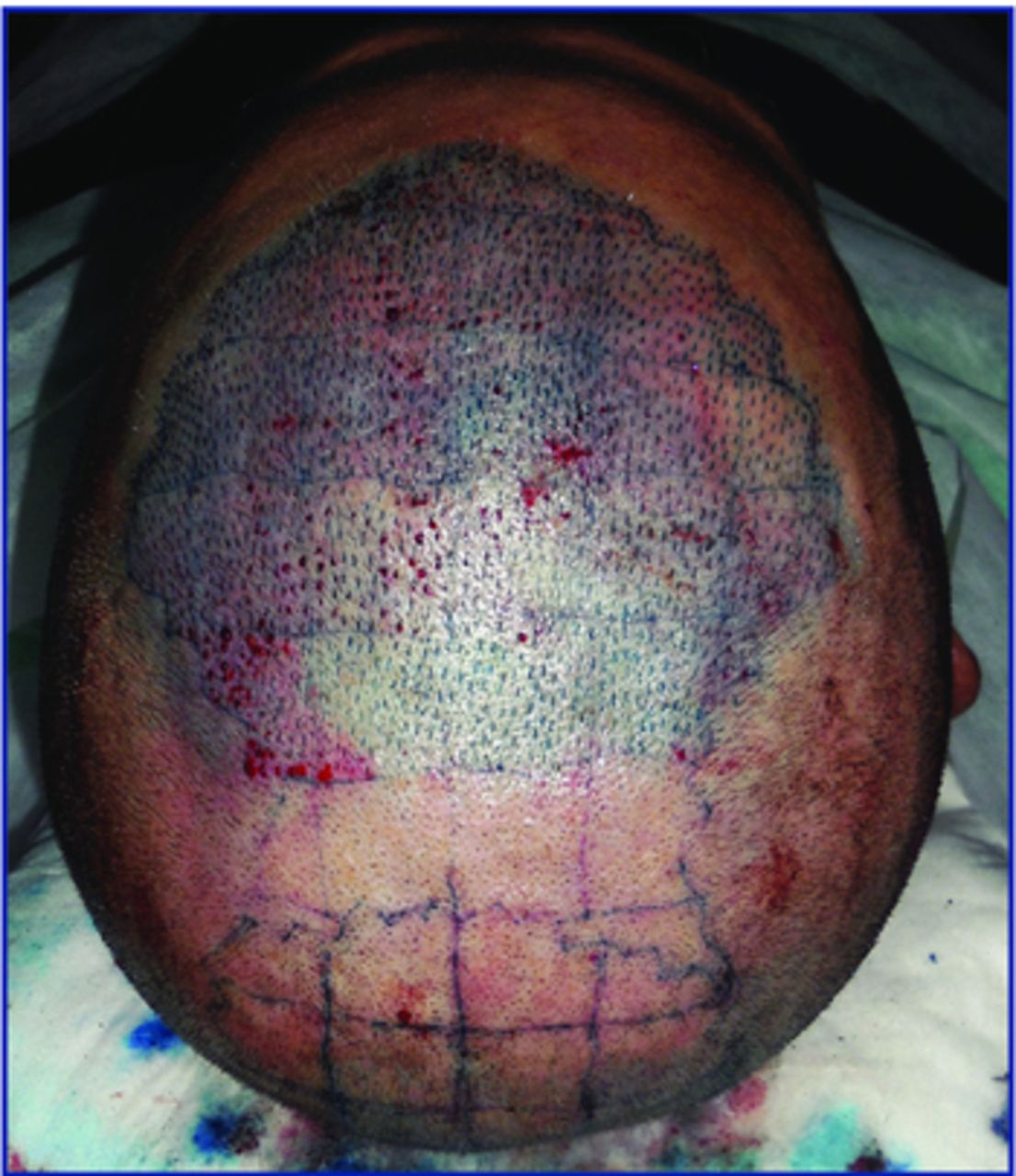
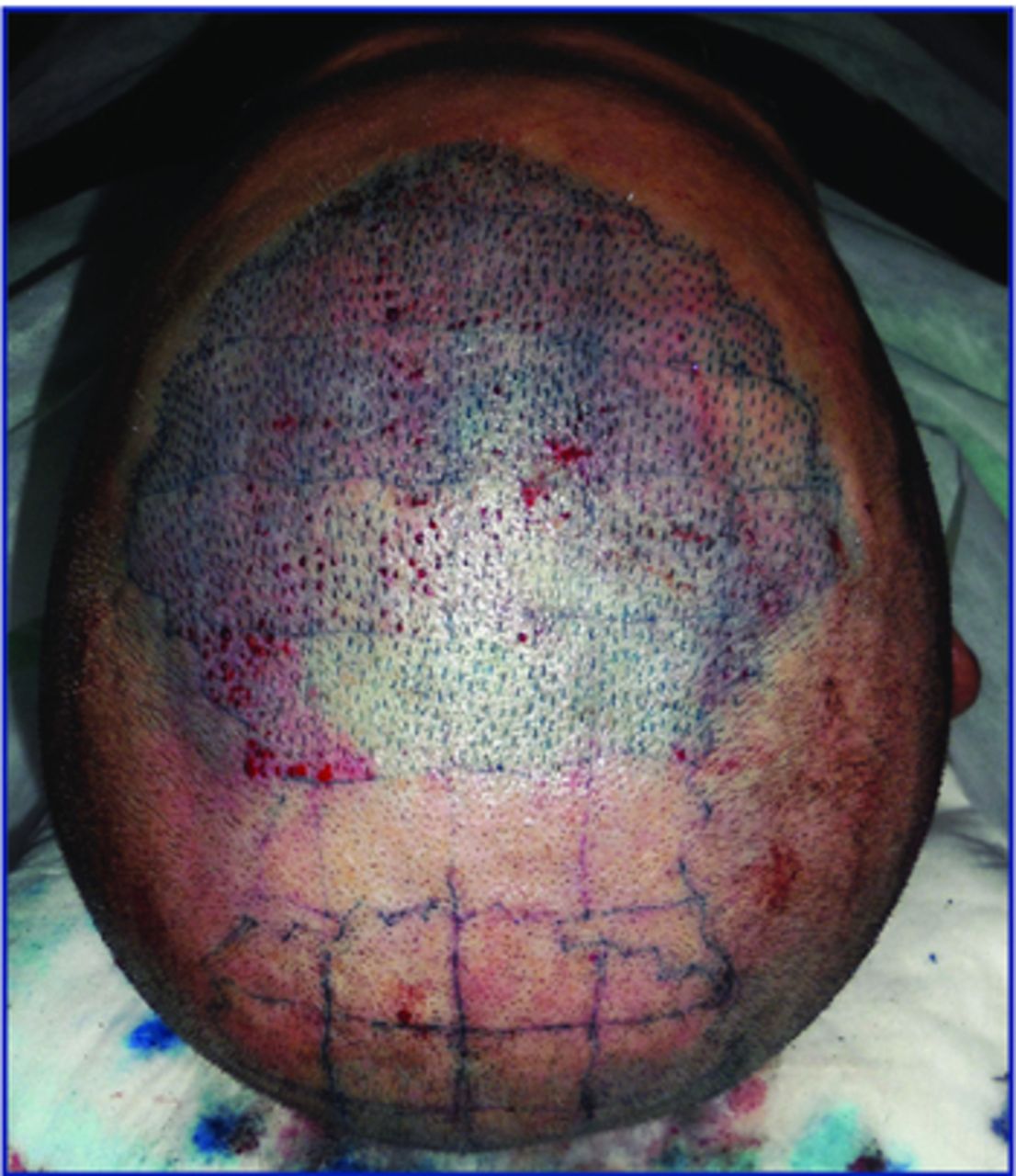
Precise density. Pre-making sites facilitates creating a predetermined density of recipient sites. We tattoo the entire recipient area and mark a grid of 2cm×2cm squares (4cm2) and make an even number of sites per area based upon the calculated desired density (Figure 9).6,7 This approach can also be used with forceps placement, but not with stick-and-place.
No replacement during surgery. With sharp needles, the implanter’s efficiency and speed are slowed as the needles get dull and must be replaced, but with dull needle implanters, these are not constraints, efficiency is maintained, and time is saved.

Lion implanters (left) and KNU implanters (right)

23-gauge needle, trimmed single hair graft, and 0.74mm dull needle implanter
8mm chisel micro blade, 2-haired graft, 0.96mm dull needle implanter

KNU needle (only steel), Lion needle (with plastic hub)
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Grid for uniform graft placement
Disadvantages
Slower. In our hands, grafts are placed at slower speed when compared to sharp needle implanters, and when compared to two or three technicians using forceps simultaneously. However, as we are gaining experience, we can have two staff placing at the same time and the process is becoming more efficient.
Bleeding and popping. In some cases, there is more bleeding and popping when compared to sharp needle implanters.
Extra care. Extra care is required to clean and sterilize dull needles for safe reuse.
Discussion
Since we started using this method, surgery has become less tiring. In FUT, the work is shared with a big team, but in FUE, the physician has much work to harvest grafts. Delegating the placement is crucial for big sessions. Because the use of forceps can more easily injure the skinny FUE grafts, the best possible solution seems to be the dull needle implanters. Since adopting them, we have seen that many hairs just don’t shed and keep growing post-operatively; something that rarely occurred when we used forceps for placement. Operating with the patient lying on his or her side is most comfortable for the patient and the entire team, and it is the most efficient as only with this positon can we harvest and place grafts simultaneously. When the patient is lying in a face up position, the physician rests while the assistant(s) place as fast as 15-20 grafts per minute each. With either approach, grafts are placed in the shortest period of time possible avoiding lengthy time out of body.
Description of the Surgical Video
Link to video:

The best way to understand the technique is to view the linked surgical video. In the online version of the Forum, simply click the link. In the print version of the Forum, either copy the link for your browser or scan the QR image above.
In the video, we show our routine doing FUE with dull needles implanters. We use the suction-assisted Trivellini Mega FUE Machine® to harvest grafts. (Editors’ note: Dr. Trivellini’s device is described in detail in a companion article in this issue of the Forum.) A 0.9mm sharp punch is our most common choice for scalp harvesting; for beard and body hair, 0.8mm is the most used. Superficial anesthesia is applied in order to get vasoconstriction and reduce the donor wound cross-section and surface area of the scalp wound.8 Punch rotation can be changed as necessary (five possible speeds). We prefer the lowest possible speed in order to harvest the grafts without damaging the bulb. When the shafts are parallel and close together in the follicular units, the punch can be inserted deeper (4mm), but when they split, 2.5 or 3mm is the deepest advisable in order to avoid transection. We punch the skin in two steps. First, the punch cuts the skin while rotating, and second, the handpiece is pressed down while the punch is not rotating in order to release the attachments and minimize transections. This makes it easier to extract the grafts with two forceps.
The suction-assisted machine has some advantages:
In case of transection, it often sucks the graft and “tells” the physician that the punch is at the wrong angle providing the surgeon the opportunity to adjust the angle, speed, and, sometimes, diameter of the punch early in the procedure, rather than discovering the transections after hundreds of grafts have been harvested.
As it sucks the blood continuously, the field is kept clean and fewer interruptions are necessary.
It frees the grafts for easier extraction at shallower punch insertion depths
Whenever possible, we punch, extract, and place grafts simultaneously, with the patient lying on his or her side. If not possible, we harvest a few hundred and then place in order to avoid long time out of the body. Our team includes two physicians and three technicians, but for smaller sessions, the work can be done by one physician and one technician.
Recipient sites can be done with needles or blades. For singles, 23g needles work well as we trim these grafts in order to have higher density in the hairline at minimal trauma. Only with this technique is it possible to place grafts into very small incisions without injuring the bulb. Incisions are always smaller than the needle diameter as the skin opening can be stretched with the dull needle. For 2- and 3-haired grafts, needles also can be used to make sites, but in our hands, blades work better. Sagittal or coronal incisions can be done. For beard transplantation, eyebrow, and temporal area, we prefer coronal, but behind the hairline, we usually prefer sagittal orientation.
The depth of recipient site incisions is exactly the length of the grafts, so before pre-making sites, we harvest test grafts in order to check their length and to make sure they fit well in the implanter and into the recipient sites.
Again, smaller incisions are done when compared to forceps and standard sharp needle implanter techniques. If the skin is elastic, 0.8mm incisions can be done for 0.96mm implanters. For more rigid skin, 0.85mm incisions are preferred.
Conclusion
In conclusion, implanters with dull needles are ideal for placement of FUE grafts because they optimally protect the grafts during insertion, can be used by assistants to place into premade sites, can be used with the smallest recipient sites, are inexpensive, and have a short learning curve to proficiency.
- Copyright © 2016 by The International Society of Hair Restoration Surgery
References
- 1.
- 2.
- 3.
- 4.
- 5.
- 6.
- 7.
- 8.