

Hair transplant surgeons have continued to refine and reproduce increased naturalness with the use of follicular units. However, many have been reluctant to rebuild temporal points fearing unnatural results.
Nordström encouraged hair transplant surgeons to avoid rebuilding the temporal points in the era of larger grafts.1 This was excellent advice in the past, and certainly the inexperienced surgeon should not attempt augmenting the temporal points. It was very difficult to get a natural result with grafts containing greater than three hairs. Unger has suggested that patients should not generally be encouraged to transplant into the temporal area because of ultimately increasing the size of the recipient area, therefore decreasing the likelihood of restoring the entire head. He also points out that it can be difficult matching the texture and caliber of hair to match the hair in the temporal recipient area.2
Khan and Stough have suggested that temporal points should not be reconstructed, but only reconstruction of the fronto-temporal triangle if there is extensive hair loss.3 Bouhanna has summarized the history of hair loss classification, but with no classification of the temporal points.4
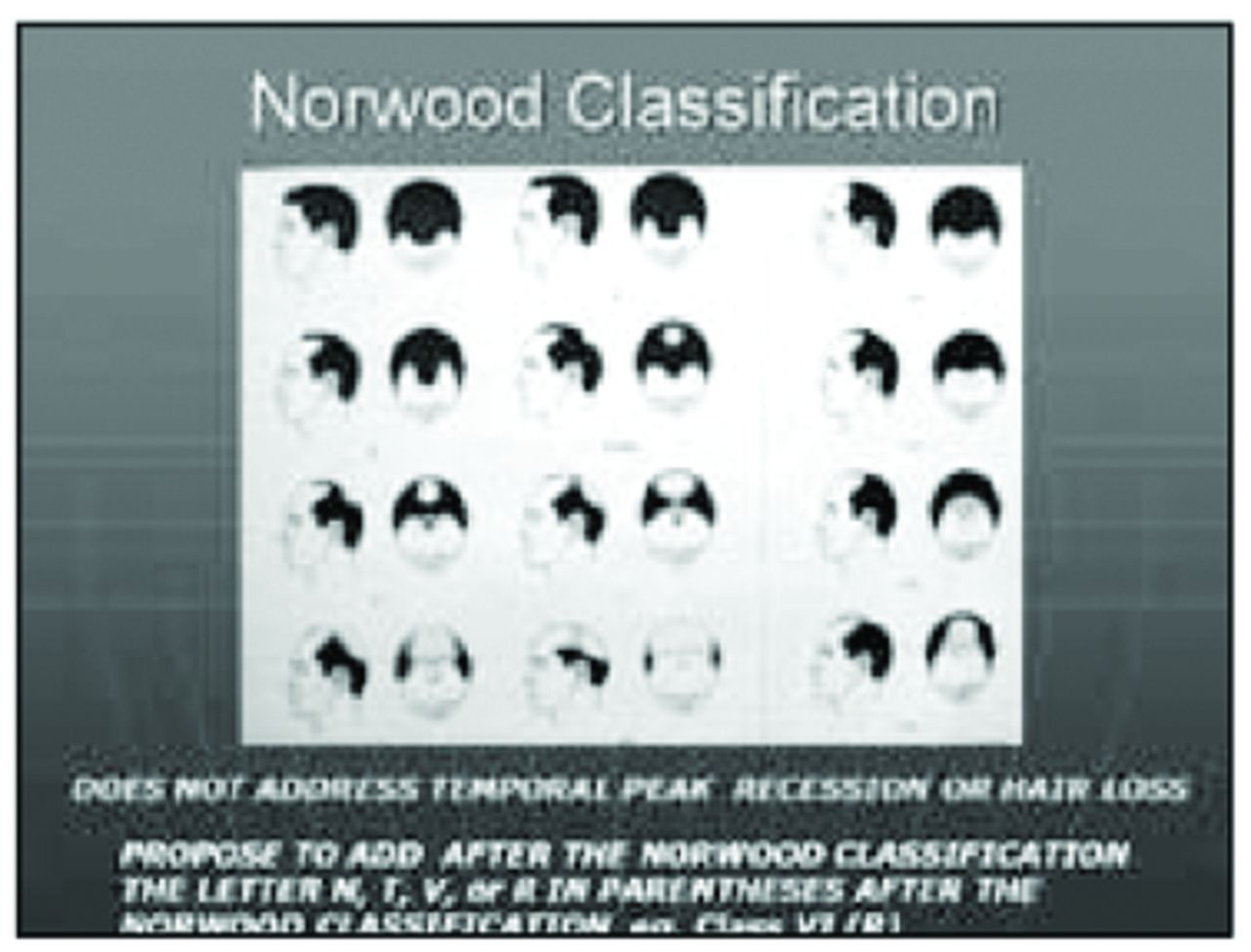
Unfortunately, there has been a delay in the surgeon’s confidence to build the temporal points. Lack of emphasis in reconstructing temporal points is also reflected in the fact that Hamilton’s Classification5 and later the more widely accepted Norwood’s Classification6 don’t address the problem of hair loss and recession of the points. Looking at this classification, one notes that all examples on the chart from I–VII have exactly the same well developed temporal points (Figure 1). One needs to add to this most popular classification an easily understood description that stages temporal point hair loss.

Norwood Classification
To describe the temporal point status, it is useful to define four following classes:
N = Normal: No thinning or recession of hair (Figure 2)

N = Normal
T = Thinning and/or mild recession (Figure 3)

T = Thinning
P = Recession is now PARALLEL to the anterior sideburn line (Figure 4)

P = Parellel
R = Recession has now caused a REVERSED angle that is usually convex, but now is concave (Figure 5)

R = Reversed angle
This straightforward classification using capital letters N, T, P, or R is added after the usual Norwood Classification in brackets to further define the patient’s current hair loss status (e.g. VI (T) or VI (P)).
Patients in class N or T usually require no augmentation. These patients should be encouraged to use Propecia® to prevent further thinning. Classes P and R should be considered for surgical augmentation. Of course, the patient’s desire is most important, but your advice is also of great value to help the patient understand the options.
After evaluating scores of “normal” temporal points, it was noted that the usual balance of the point with the frontal hair line is the location where the following two lines bisect (Figure 6). Line 1 is drawn from the most anterior portion of the frontal hair line to the tip of the ear lobe. Line 2 is drawn from the tip of the nose, over the center of the pupil, and extended to the temporal point. Where the two lines bisect is an excellent reference point to place the anterior tip of the temporal point.

Bisection of Lines I & II
Never allow the above “rule of thumb” to override your own artistic judgment. Learn to look at the shape of the head along with the balance of the eye, ear, and nose aesthetics. And, of course, never forget the patient’s desires and restoration goals. One must always remember that hair loss is progressive, and you must put the patient in a “time machine” envisioning the patient 30–40 years hence.
Surgical techniques are similar to transplanting eyebrows. After the design is drawn with a black grease pen, a surgical marker is used to place irregular dots outlining the proposed temporal point. This won’t be rubbed off when the anesthesia is introduced or when the area is cleansed with an antiseptic.
The best match of color and caliber is usually located in the supra auricular or the supra post-auricular area (Figure 7). It is imperative to match the color of the transplanted hair to that of the hair in the receding temporal point or you will create a very unnatural appearing point. It is better not to build out the point if you don’t have matching hair color available.

Supra auricular hair best donor
Because the best match of hair color and caliber is supra auricular, when taking the donor strip, extend your planned incision to include hair from this area. Always remember to leave the hair at least 1cm long (Figure 8). This will ensure that the curl and hair direction will be more easily determined when placing the follicular units into the recipient area (Figure 9).

Keep hair 1cm long.

Curl down and in toward the skin.
Planning the amount of donor hair for the points is done by calculating the area to be restored in square centimeters. Twenty to 30 follicular units per square centimeter is a reasonable goal. Usually about 125–150 follicular units are required per side. Use only one- and two-hair grafts, and place only the naturally occurring single follicular units at the edge (Figure 9).
When making the sites, always place the bevel of the blade flat to the surface of the dermis. The recipient sites in the edge are best made with a solid core 18 gauge needle (Figure 10A). The singlehair follicular units fit well into these sites. More central to the point, behind the singles, an SP 90 blade laid flat to the skin surface creates an excellent site for the two-haired follicular units (Figure 10B).

Solid core 18 gauge bevel flat to the skin

SP 90 blade flat to the skin
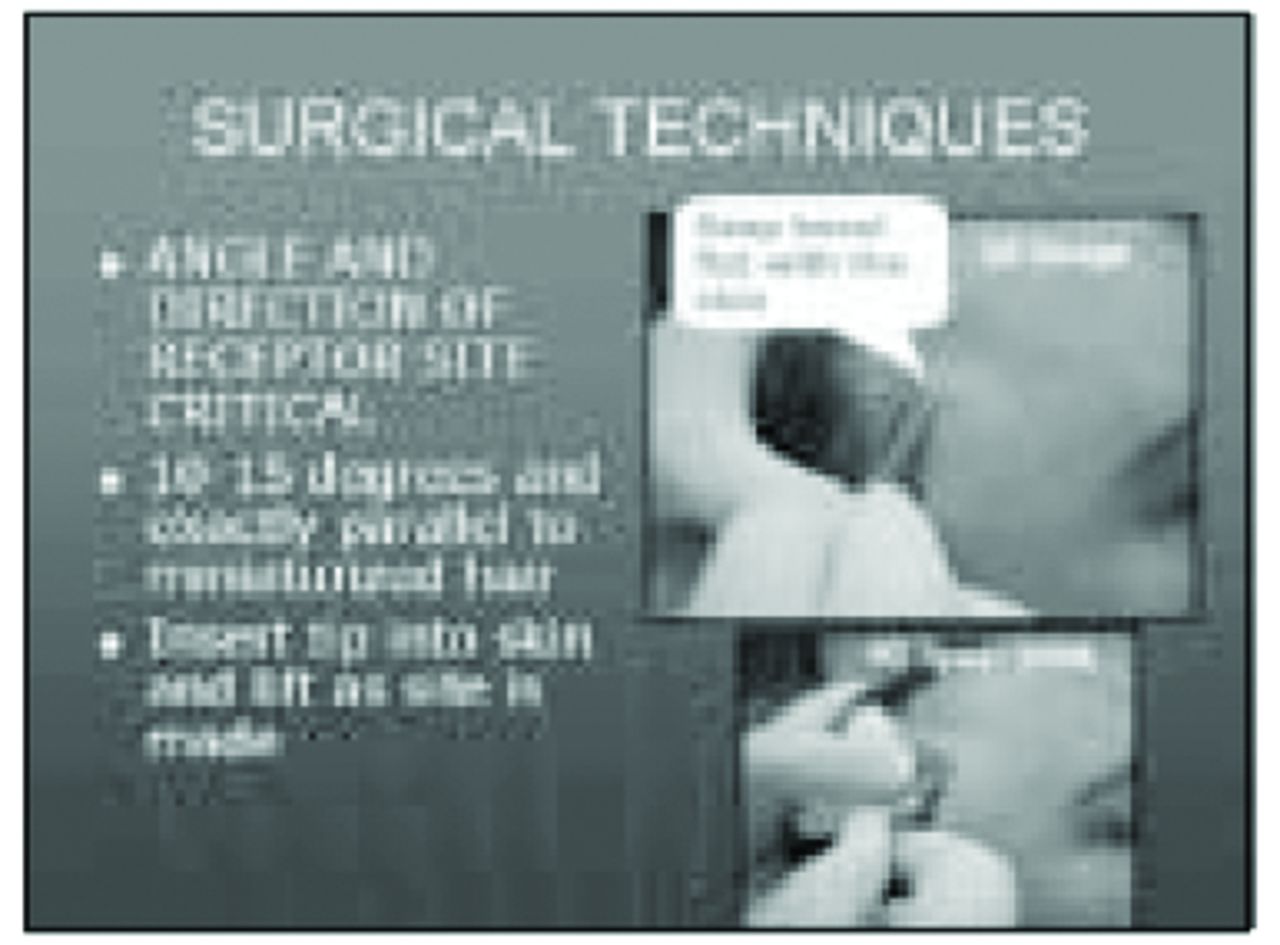
To reproduce nature, observe that the hair in the points grows at a very acute angle downward and posterior. Also, there are usually a few miniaturized or vellus hairs that can be used as a template to duplicate the correct angle. Keep the needle or blade as flat as possible to keep these angles acute. The skin must be kept tight with your index finger and thumb as the sites are created with your other hand (Figure 11).

Hair grows at acute angle downward and posterior.
The dressing that is very useful is a 4 inch square piece of Vigilon cut diagonally leaving two triangles that fit perfectly over the temporal points. Place gauze over the Vigilon followed by a Kerlex wrap to keep the patient from rubbing the grafts out from friction of the pillow.
Despite using post-op glucocorticosteroids, there is increased probability of periorbital edema and possibly even ecchymosis when building out the temporal points. Always remind the patient of this possibility, which occurs 30–40% of the time usually 3–5 days post-operatively.
By using the above classification, patient evaluation, artistic considerations, surgical techniques, and postoperative care, the transplant surgeon can augment the temporal points with confidence and obtain a natural result (Figures 12, 13, and 14).

Before and After

After

Immediately post-op

Post-op 2 sx

Post-op close-up
- Copyright © 2002 by The International Society of Hair Restoration Surgery
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.