


While transplantation is the cornerstone of our collective practices, medical therapy directed at mitigating ongoing thinning and subsequent loss is of critical importance in addressing our patients’ quality of life concerns related to the cosmetic appearance of overall hair density and/or fullness. At the most recent International Congress of The Brazilian Society of Hair Restoration Surgery held in Maresias, Brazil, I and my ISHRS colleagues in attendance appreciated Dr. Piero Tesauro’s presentation on his approach to medical therapy in the treatment of male and female pattern hair loss. Below, Dr. Tesauro details the treatment modalities he uses in his daily practice.
This article presents an approach utilized in our clinic employing galenic therapy for the medical management of commonly treated alopecias. Galenic therapy is defined as the use of prescription drugs not generally available directly to the public but that are prepared in a laboratory as requested by a physician or medical practice (this is also known as compounding). These compositions are a custom ensemble of individualized prescription medications that can be administered topically or orally. Following are examples of topical galenic therapies used to address commonly seen alopecias along with the subsequent clinical outcomes observed as a result of consistent use of each therapy.
Premise
The hair cycle is controlled by the circulating steroidal sex hormones that are metabolized by the follicle itself. Control of this hormone production can slow hair loss (Figure 1).

Androgen metabolism of the pilo sebaceous complex.
Pattern 1: Androgenetic Alopecia (AGA)
AGA is supported by a multigenetic family inheritance, the presence of androgen hormones in the plasma, and in particular the activity of the 5-alpha reductase enzyme in the hair follicle. The 5-alpha reduction of testosterone to dihydrotestosterone is in fact associated with the thinning of the hair on top of the head and a coincident retraction of the frontal hairline, both typical of AGA. Finasteride, which inhibits the enzyme 5-alpha reductase, type II, is used for oral therapy in these cases while minoxidil and progesterone are the topical therapy options:
ORAL THERAPY
Finasteride 1mg/Day
TOPICAL THERAPY:
Minoxidil 2%
Progesterone 1%
Transcutol 5%
Alcohol 80% to preference to adjust viscosity and drying
Distilled water to a volume of 200ml
Minoxidil. The second FDA-approved drug for the treatment of baldness is a peripheral vasodilator in which its capacity to stimulate the growth of hair was discovered around 1980. The mechanism of action of minoxidil is not yet clear. Pre-clinical studies suggest that minoxidil slows cellular senescence in a similar way to how the epidermal growth factor (EGF) prolongs the anagen phase of the hair growth cycle. This active principle seems to mimic the action of a growth factor stimulating the mitosis of the matrix.
Progesterone. Progesterone for local use inhibits the activity of 5-alpha reductase by competing with testosterone and reducing its conversion into dihydrotestosterone. Progesterone reaches the epidermal, dermal, and glandular tissues and is then metabolized in the pilosebaceous complex into an inactive derivative. Systemic absorption is not observed in clinical use.
Transcutol. Highly purified diethyene glycol monoethyl ether EP/NF is an agent that improves skin penetration of a drug. Safety has been demonstrated by extensive toxologic evaluations and it is used in approved pharmaceutical products. The lotion is less greasy. Transcutol does not have a long shelf life.
Pattern 2: Estrone Deficiency
A widespread clinical hypotrichia with centrifugal patterns corresponds to a type of alopecia called “estrone deficiency” (Dr. Andrea Marliani). Histologically, the hair in these cases decreases in its diameter but does not lose its follicular depth. It is assumed that this condition is in fact linked to a deficiency of estrone and in turn is connected to a possible reduction of activity of the enzyme aromatase and/or 3-alpha reductase. Therapy to address the mechanism in these cases is restricted mainly to topical corticosteroids:
Hydrocortisone butyrate 0.05%
Estrone basis 0.05%
Transcutol 5%
Alcohol 80% to preference
Distilled water to a volume of 200ml
Hydrocortisone butyrate (Cortisol). Activates neoglicogenesis in the cell matrix and papilla of the hair bulb and allows for the production of glycogen to ensure glucose homeostasis and energy of the hair. The use of a mild corticosteroid is also useful for controlling the erythema and desquamation, thus putting the skin in a condition to better receive the other topical therapies. A further property of that active ingredient is to counter the phenomena of fibrous scarring that occurs in all trichological pathologies leading to the permanent loss of the follicle.
Estrone basis. The estrone activates the enzyme adenyl cyclase activating glycolysis, with the production of energy in the form of ATP, and therefore promotes the mitosis of the cells of the matrix and the papilla. This hormone is therefore not only responsible for the maintenance of the anagen phase, but also the activation of bulge stem cells.
Pattern 3: Mixed Clinical Patterns
Mixed clinical patterns of AGA and estrone component deficiency are usually treated with the following formulation:
Minoxidil 2%
Progesterone 1%
Hydrocortisone butyrate 0.05%
Estrone basis 0.05%
Example of a prescription and its directions for use:
Galenic lotion for topical use:
Minoxidil 2%
Progesterone 1%
Hydrocortisone butyrate 0.05%
Estrone base
Transcutol 5%
Alcohol 80% to preference
Distilled water to a volume of 200ml
METHOD OF APPLICATION
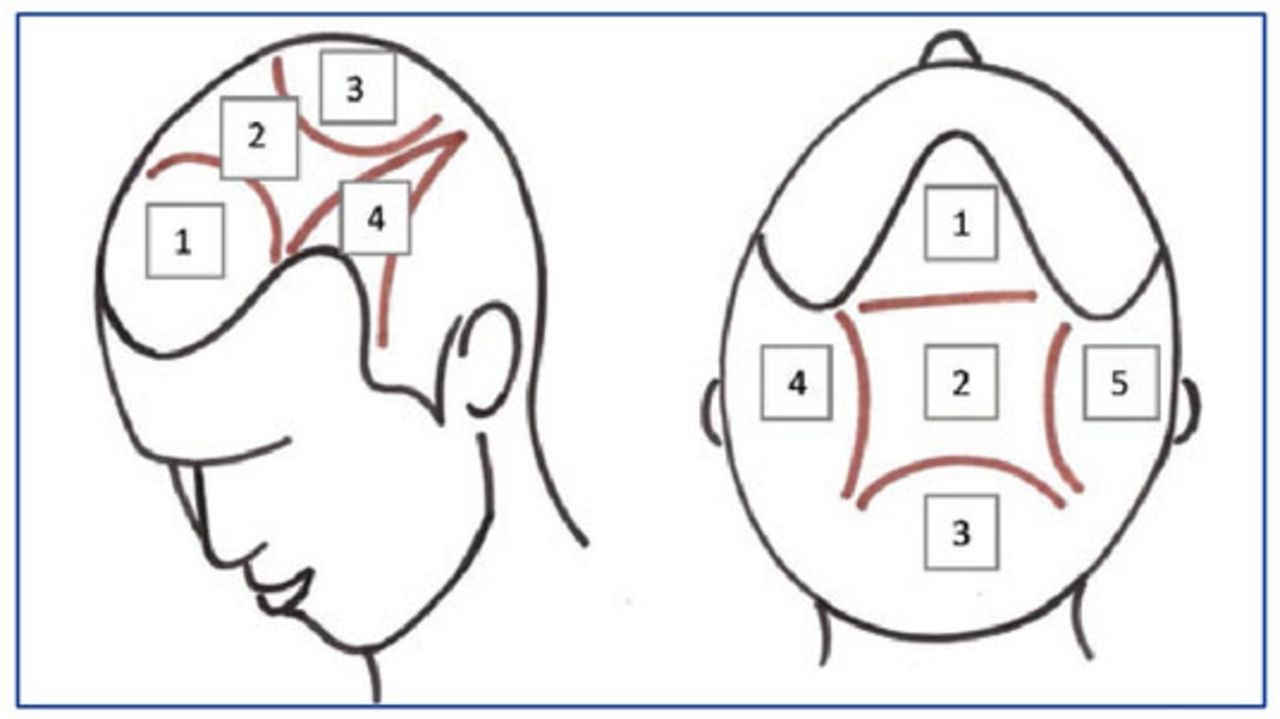
In Pattern 1, the lotion is applied twice daily as usual (2ml). In Patterns 2 and 3, for many years we have used a different protocol of applying the lotion all over the scalp as follows (Figure 2):

Application of the lotion: 1, frontal area; 2, central area; 3, vertex area; 4, left parietal/temporal zone; 5, right parietal/temporal zone.
INSTRUCTIONS
Apply 5ml of lotion (about 100 drops), 3 times a week on alternate days (e.g., Monday, Wednesday, and Fri-day) after shampooing.
The lotion should be applied to the following 5 areas of the scalp, 1ml (20 drops) at a time: 1ml on the frontal area, 1ml on the central area (the area between the front line and vertex), 1ml on the summit, 1ml on the right temporal/right parietal zone, and 1ml on the left temporal / left parietal zone.
Massage for 30 seconds with the fingertips to help the absorption of the lotion per ml used.
In summary: Run the shampoo; dab your hair with the towel; apply the lotion on the 5 areas of the scalp, massaging each part for 30 seconds after each ml applied; blow-dry your hair.
Examples of Pattern 2 clinical cases are shown in Figures 3, 4, and 5. Examples of Pattern 3 results obtained with galenic lotion in association with oral serenoa repens (saw palmetto) and finasteride are shown in Figures 6, 7, and 8.

Pattern 2 patient (estrone deficiency): before (left) and after (right) 2 years of treatment.

Pattern 2 patient (estrone deficiency): before (left) and after (right) 1 year of treatment.

Pattern 2 Patient (estron deficiency): before (left) and after (right) 2 years of treatment.

Pattern 3 patient progression over 13 months. Galenic lotion and oral serenoa repens and finasteride 0.25mg.

Pattern 3 patient: before (left) and after (right) 7 months (June 2013–January 2014). Galenic lotion and oral serenoa repens and finasteride 0.25mg.

Pattern 3 patient: before (left) and after (right) 9 months (July 2013–March 2014). Galenic lotion and oral serenoa repens and finasteride 0.25mg.
It is often necessary in my clinical practice to use a reduced dose of finasteride (0.25mg.). Patients are often frightened by the use of Propecia® and dosage reduction is extremely soothing. While I have a feeling that the reduction of the dose (0.25) reduces side effects, I’m certain that it greatly reduces the nocebo effect.
We know that the efficacy of finasteride was demonstrated at doses of 0.2mg/day or higher. We also know that 1 and 5mg doses are of similar efficacy but somewhat superior to lower doses.
Although I agree that the use of a combination of finasteride and saw palmetto can be controversial, I consider three good reasons to do so:
Serenoa repens strengthens the anti DHT finasteride action.
The saw palmetto acts on 5-alpha reductase receptors type 1 and type 2.
Many of the most popular over-the-counter supplements contain the serenoa repens in combination with other substances (minerals, vitamins, natural anti-inflammatory and antioxidants), which probably have a different mechanism of action than the finasteride itself. When I perceive the utility of these supplements, I will always include the serenoa.
I understand that these reasons are not supported by scientific clinical research as that would require a dou-ble-blind study. I hope soon to take a step forward in this direction but for now this is exactly is “How I do it”… with good results!
- Copyright © 2014 by The International Society of Hair Restoration Surgery
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.