

Androgenetic alopecia (AGA) affects both genders and is characterised by hair loss in a distinctive and reproducible pattern from the scalp.1 Local and systemic androgens transform large terminal follicles into smaller vellus-like ones.2 Follicular miniaturization is the histological hallmark of AGA.3,4
Diffuse hair thinning and increased hair shedding precede the appearance of baldness by a number of years. This is because the follicular miniaturization of AGA does not simultaneously affect all follicles within a follicular unit (FU). Instead, there is a hierarchy of follicular miniaturization with a follicular unit’s secondary follicles affected initially and primary follicles miniaturized last.5
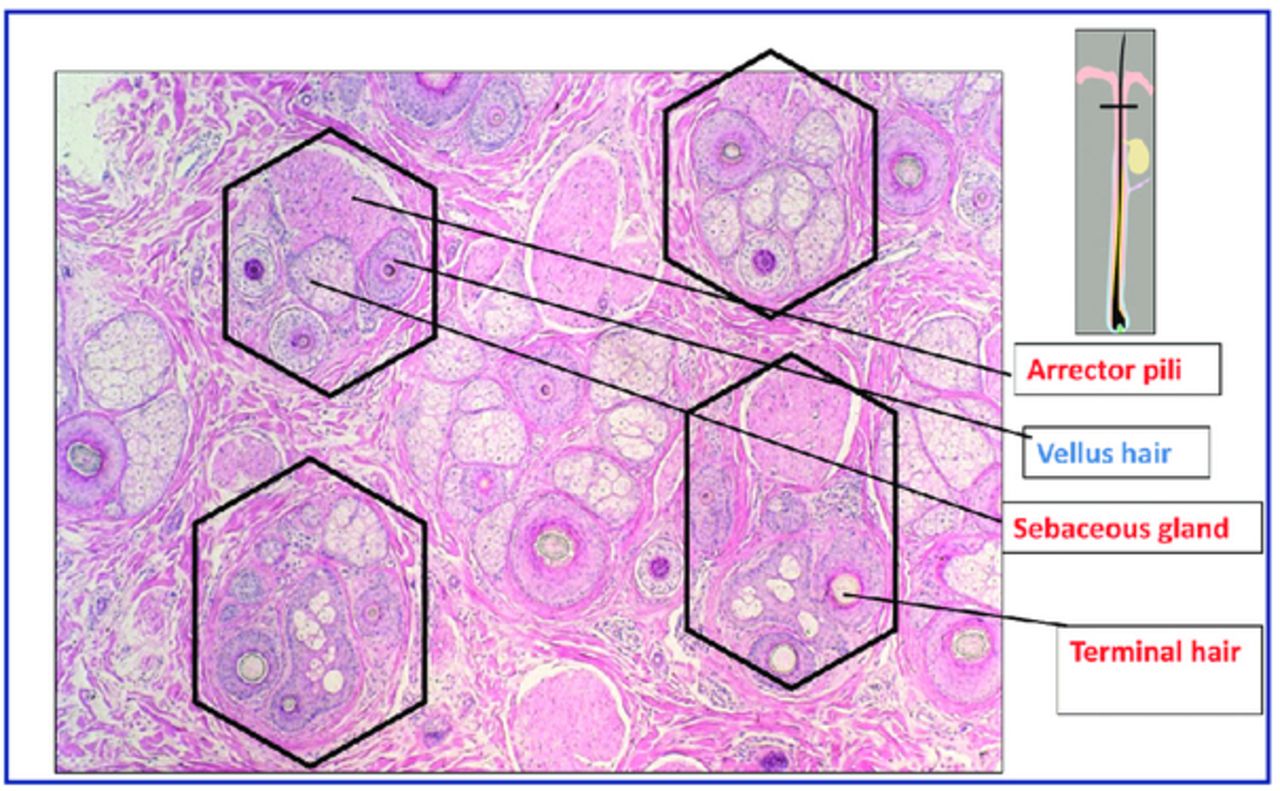
Scalp hairs arise from FUs that are best seen on horizontal scalp biopsy. FUs comprise a primary follicle that gives rise to an arrector pili muscle (APM), a sebaceous gland, and multiple secondary follicles that arise distal to the APM (Figure 1). Hairs from secondary follicles commonly emerge from a single infundibulum (Figure 2). In contrast, hairs over the beard, trunk, and limbs do not give rise to secondary hairs and exist singly or in groups of 3, known as Meijeres trios (Figure 3). Miniaturization occurs initially in the secondary follicles, leading to the reduction in hair density that precedes visible baldness (Figure 4). Baldness ensues when all of the hairs within a FU are miniaturized.

Horizontal section of skin biopsy from a hairy scalp showing features of early androgenetic alopecia. Follicles exist within follicular units comprising arrector pili muscle, sebaceous gland and derived secondary hairs, some of which have miniaturized to become secondary vellus hairs.

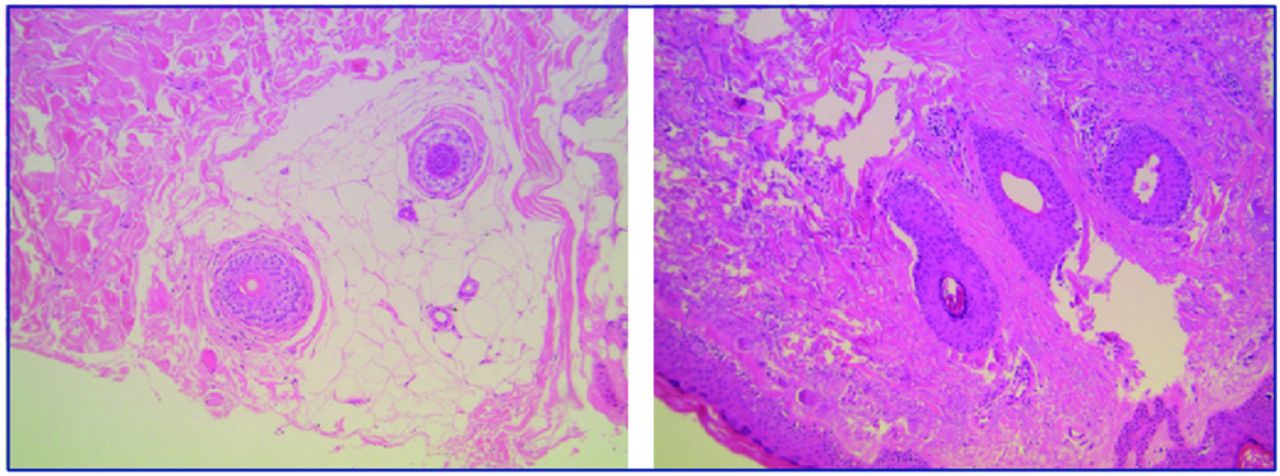
Multiple hair fibres can be seen to emerge from a single infundibulum.

Horizontal section of skin biopsy from a hairy forearm showing follicles to exist singly (left) or in groups of 3 (right), known as Meijeres trios.

In AGA, there is a reduction in the number of hairs per FU that precedes the development of baldness.
One vexing question is that identical hair follicle miniaturization is seen histologically in lesions of alopecia areata. In this condition, miniaturization of all follicles occurs simultaneously. Unlike AGA, miniaturization in alopecia areata is potentially fully reversible.
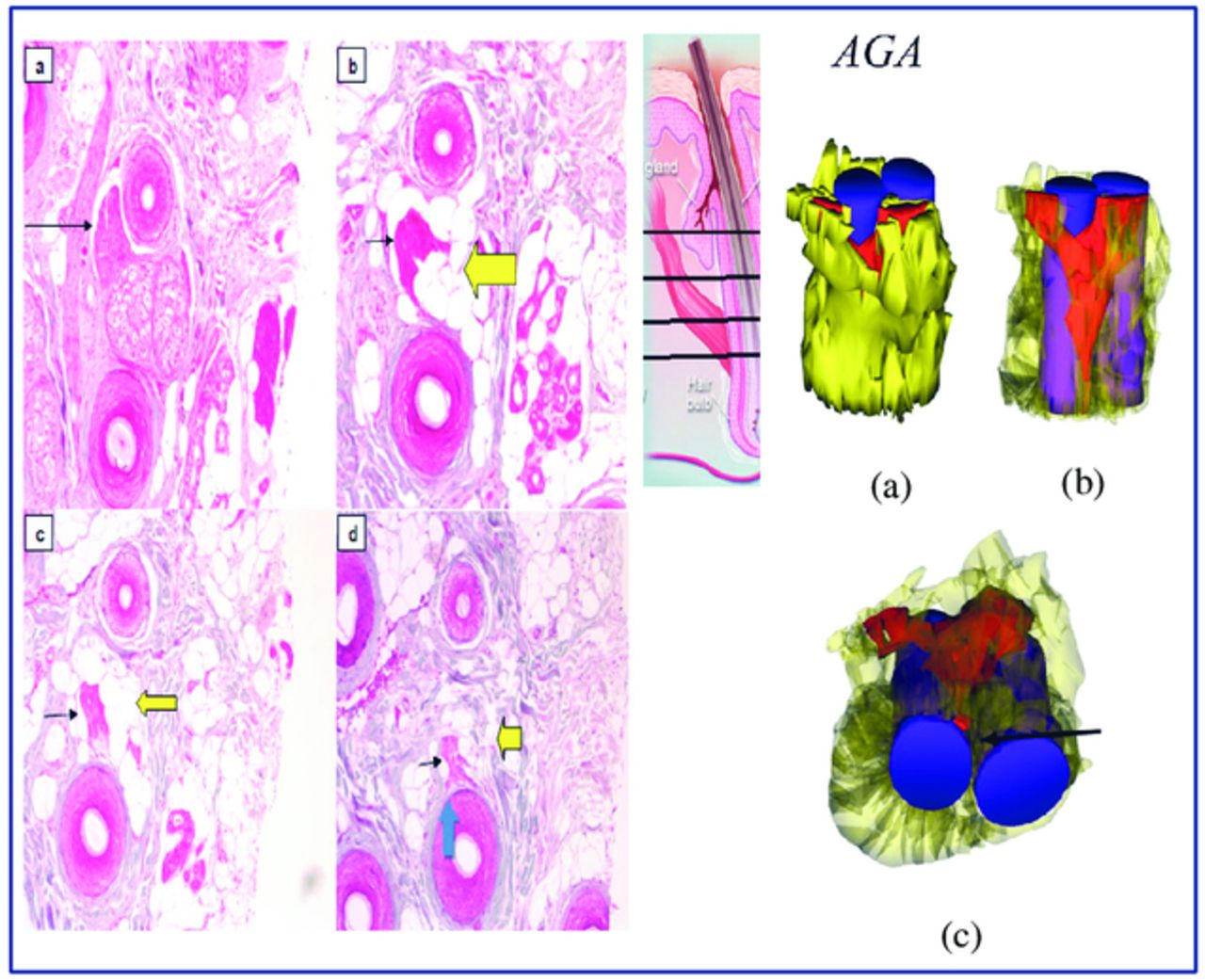
This apparent paradox can be explained by investigation of the arrector pili muscle (APM) and in particular its proximal attachment to the hair follicle bulge.9 The APM is a small band of smooth muscle that runs from the hair follicle to the adjacent upper dermis and epidermis. This muscle contributes to thermoregulation and sebum secretion. The APM arises proximally at the hair follicle at the bulge, which is an epithelial stem cell niche. Three-dimensional reconstructions of scalp biopsy specimens demonstrate that preservation of the APM predicts reversible hair loss (Figure 5) and conversely loss of attachment between the APM and hair follicle bulge is associated with irreversible or partially reversible hair loss (Figure 6).

In telogen effluvium and also alopecia areata, the arrector pili muscle (red) can be shown to be attached to the hair follicle (purple).

In androgenetic alopecia, the proximal arrector pili muscle (red) is progressively replaced by adipose tissue (yellow) and loses its attachment to the hair follicle bulge (purple).
The APM plays a significant role in maintaining hair follicle integrity. Restoration of the APM in transplanted hair follicle units has been shown to induce the regeneration of the neurofollicular and neuromuscular junction in the follicle bulge in single follicular unit transplant in androgenic alopecia patients.7

Reduction in dermal papilla cell numbers as an indirect result of changes to the dermal sheath. The sheath cells (solid cells) that surround the follicle are an integral part of the follicle dermis (a). If they are functionally lost (dotted cells arrowed) from the follicle (b), then dermal papilla cells (outline only) move from the papilla to replace them (c). As a result, the papilla and the follicle become smaller. (Reproduced from: Jahoda C. Cellular and developmental aspects of androgenetic alopecia. Exp Dermatol. 1998; 7:235-248.)
The discovery of progressive muscle volume loss and fat infiltration in AGA samples that was associated with total or near to total loss of the muscle attachment to the primary follicle bulge8 led to the hypothesis that maintenance of the attachment between the APM and the bulge might differentiate between reversible and irreversible hair follicle miniaturization as these features were exclusive to AGA. The finding that the APM is preserved in telogen effluvium and alopecia areata supports this view.

Scalp follicles exist as compound follicular units. In AGA, miniaturization occurs initially in the secondary follicles. This leads to a reduction in hair density that precedes visible baldness. Bald scalp only becomes visible when the all of the hairs within a FU are miniaturized. With miniaturization, the muscle initially loses attachment to the secondary follicles. When primary follicles eventually miniaturize and lose muscle attachment, the hair loss becomes irreversible.
It appears likely that the interaction between the mesenchyme-derived APM and the follicle bulge epithelium is essential for the integrity of the pilosebaceous unit, much in the same way as the interaction between the mesenchymal-derived dermal papilla and the epithelial hair follicle matrix.
Follicle cycling is associated with the movement of cells between the dermal papilla and dermal sheath.10 It is thought that disruption of this process in AGA causes a loss of cells from the dermal sheath and then the dermal papilla that consequently leads to hair follicle miniaturization (Figure 7). Cells from the dermal papilla and dermal sheath are capable of undergoing both smooth muscle and adipose differentiation in vitro. Cells from the follicle mesenchyme might also contribute to maintenance of the APM, and the muscle degeneration seen in AGA could be caused by the loss of a progenitor cell population that maintains both the APM and the dermal papilla.
In conclusion, we propose a new model for AGA (Figure 8). In early stages of hair loss, the arrector pili muscle remains attached to the primary follicle, but loses its attachment to some of the regressing secondary follicles in some follicular units. Miniaturization of secondary follicles and detachment of the APM from these follicles extends to the rest of the follicular units. At this stage, patients may complain of hair thinning and loss of volume in their ponytail without any visible baldness.
With further progression, miniaturization continues and the muscle loses attachment to the secondary follicles in affected follicular units completely. Primary follicles eventually miniaturize and this leads to visible baldness. When primary follicles lose muscle attachment, the hair loss becomes irreversible. Hopefully this model facilitates a clearer understanding of normal hair growth and also hair loss conditions.
Editor’s note: I asked Professor Sinclair why dermal papilla cells are lost to the dermal sheath at cycling resulting in a smaller papilla and therefore a smaller hair. What is it that makes them move out? It seems that if we can identify the process here, we may be able to reverse that process. We know that a larger dermal papilla equals a larger hair.
He quoted from Jahoda: “Reduction in dermal papilla cell numbers are an indirect result of changes in the dermal sheath cell numbers. The sheath cells that surround the follicle are an integral part of the follicle dermis. If they are lost from the follicle during catagen or telogen, then dermal papilla cells will move from the papilla to replace them at the onset of anagen. As a result the papilla and follicle become smaller.” (Jahoda, C. Cellular and developmental aspects of androgenetic alopecia. Exp Dermatol. 1998; 7:235-248.) Maybe the dermal sheath will give us some answers in due course.
Also, we know that FUE aficionados are now refining the harvesting process by only partially harvesting an FU, that is, leaving behind one hair of a multiple FU. This way there are no gaps left in the donor area. Professor Sinclair talks of primary and secondary follicles so the question is, if the primary follicle is taken, would the secondary follicles left behind perish? Conversely, if only secondary follicles are taken, will they grow without their primary hair?
He replied that there is a risk of damage to the remaining follicle in partial harvesting of a follicular unit, but he felt that the primary/secondary follicle concept should not affect growth. —MM
Editor’s note: What appears to be an FU on the surface of the skin may actually be one or more FUs. We are in the age of sub-follicular unit grafting not only in FUE but also because cutting down FUs has been very widespread with FUT for several years.
Actually, in its most contemporary iteration, FUE is done with fractional harvesting. We look for clusters of hair (usually more than 1 FU) and split off the tightest groups leaving the other hairs in the cluster. Very often, actual FUs are not split apart, though sometimes they are, but it is a misconception to characterize current FUE as associated with routine splitting of follicular units. —RHT
Note from Dr. Jerry Cooley: In this paper, Drs. Sinclair and Torkamani report that in androgenetic alopecia the arrector pili muscle (APM) is lost and replaced with fat as balding progresses. There is both a practical and theoretical outcome to this finding. It is sometimes hard to distinguish androgenetic alopecia from other non-scarring alopecias, such as chronic telogen effluvium. A biopsy showing loss of the APM and replacement by fat would certainly suggest AGA; it might be worthwhile asking our dermatopathologists to start looking for this in the biopsies we send them.
Theoretically, detachment of the APM from the hair follicle may represent the “point of no return” when a miniaturizing follicle can no longer be medically revived (e.g., finasteride, minoxidil) and will progress to the vellus state. To bolster this theory, it would be nice to see sequential biopsies over time in patients on medical therapy, looking specifically at the APM attachment to the follicle. While it may be hard to carry out such a study, it would help prove that APM detachment is irreversible and lend considerable support to this new theory.
- Copyright © 2015 by The International Society of Hair Restoration Surgery
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.