

Concealers have been used for decades by men and women to camouflage their balding and thinning scalps. Although previous use of cosmetic tattoos have been attempted by cosmetic service providers,4 not until recently has this become an art form used by cosmetic surgeons.1,2,14 SMP reflects the use of permanent concealers in the form of a specialized tattoo applied in a stippling pattern to mimic closely cut hairs. It has been applied to a wide variety of pathologies of the hair and scalp in hair restoration surgeons’ offices and even in tattoo parlors. A special cosmetic tattoo instrument with a handpiece that utilizes reciprocating needles is used to apply the stippled pattern between the pores of the scalp. The dot size must be small, around 0.1mm as seen from the surface of the skin (Figure 1).

Close-up of dots
Equipment and Inks (Pigments)
The equipment is standard for cosmetic tattoo instruments, containing one or more needles. These machines vary in costs from US$1,000-$3,500. Needles cost approximately $10/use and are disposable. The handpieces are part of the machine costs. In our hands, we use only organic pigments that contain no heavy metals unlike many tattoo inks. When it comes to the color of the inks, we always tell our patients that we use 50 shades of gray, which is close to the truth as we dilute black ink to achieve many shades of gray. Hair that exits the scalp is usually gray so what we do is not so different than what Mother Nature does.
The limited donor supply of hair for the advanced balding pattern patient often creates a problem for the patient and the doctor. For example, for those with low donor density and a Class 4 or 5 pattern or greater, the ability to cover the balding area with hair transplantation alone is limited. This is particularly relevant for the Asian patient with generally 20% less available hair for transplantation. SMP, in combination with hair transplants, offers a solution not heretofore available. When fine dark hair and a light skin color appear in combination, as it does in many Asians, the low Asian donor density complicates surgical planning. SMP, therefore, allows the doctor to achieve the patient’s desired results with less grafts.
SMP is uniquely suited to a variety of conditions for which there is no other alternative such as 1) the punctate scars from FUE, 2) those with see through donor areas when extractions are above the 4,000-5,000 level, and 3) in those patients with lower than normal donor densities. Previous hair transplant patients who have become heavily donor depleted, often with significantly scarred donor areas, are ideal candidates for SMP, and it offers the patient an ability to achieve a normal looking donor area without further hair transplantation as SMP addresses the scarring and see through donor areas directly.
The SMP process is paradoxically both easy and difficult. A cosmetic tattoo handpiece contains more than one needle that cycles between 120-150 cycles per second, penetrating the epidermis with each cycle. The inks (pigments) are passed into the wounds by surface tension between the needles. As such, the amount of ink delivered is non-quantitative and the multiple insertions delivering the ink through surface tension work as a two way street (upward and downward), delivering only a small amount of ink past the epidermis into the dermis. As the depth of the delivery is hand controlled, depth control can become a real problem. Too deep delivers an amalgam of ink that appears blotchy, too superficial, the ink does not get into the dermis and leaks out as each needle withdraws. If held too long in the dermis, too much ink gets delivered, and if not passed beyond the basement layer of the epidermis, an inadequate amount of ink is delivered. To compound the problem of ink delivery, the cycling needles produce a significant wound in the epidermis that leaks ink out of the wound while it is being done as to obscure the visual field. Depth control becomes a tactile skill that takes millions of passes to get it right, so the skill required is a time-consuming, tedious process. In each procedure, it may take over 50,000 insertions to create the stippled pattern, and this usually takes all day. For every wound, if the ink is implanted in inadequate amounts, at too superficial a depth, or if the ink should be “attacked” by the body’s immune system, a second pass is almost always required. What your eye sees during the SMP process may not reflect the ink delivery into the proper depth. Usually, in our hands, an average of three passes on each patient is required, sometimes more, rarely less, and always at least 1 week apart. Perfection for performing SMP on an entire head might take 20-30 hours of work over a few days separated each time by a minimum of one week. Occupational hand and wrist injuries are common in the operators so frequent rest periods are essential.
The inks come in two general varieties: temporary or permanent. Temporary inks make no sense as they may start to fade fairly quickly, sometimes as early as months after the process occurs. As it takes considerable time to put the ink in, losing the ink in a few months does not impart a real benefit for the patient over any reasonable time frame. The cost to perform it is high, too high for a temporary process that has to be repeated in less than a year. The permanent inks reflect the lifetime tattoos we see in body art, so the impetus for the operator to get it right in as few sessions as possible is high. Over-shooting requires laser removal of the inks, a real problem for the physician’s practice and in generating patient satisfaction and confidence. We have been doing permanent SMP for 6 years and on many hundreds of patients, and not one patient has regretted it. I take this to mean that we did not “sell” the patient on the process, we educated them well and then the patients were thrilled to achieve their targeted results predictably.
Some people are concerned about a bluish tinge of the inks on the skin. This slight color is there, worse if you use a dark black ink than a shade of gray. This has not been a problem with our patients, but if you look carefully on some of our SMP patients, you may see a blue tinge. The veins on the back of my hand are green, but I can assure you that my blood is as red as the blood of all of our readers, so what we see is the absorption of light that impacts the colors we see. This is the case with the darker inks used for SMP.
The SMP is performed under local anesthesia using a ring block just as we do with a hair transplant, but because the work is very superficial, the block does not require the depth of the nerve block as what would be a typical hair transplant anesthesia technique. A few patients are willing to do SMP without anesthesia, but those numbers are very few.
Patient education and marketing: Educating the patient is critical. We spend an average of one hour in each consultation for the education process. The good news is that most hair transplant doctors have patients in their databases with donor area scars, thinning with unachieved fullness, and people whose hair loss has progressed since the hair transplant was done. As these patients return to you, this is an excellent opportunity to present this new modality for addressing their problems. Good internal marketing campaigns are easily undertaken to secure your initial patients for an SMP offering. I would generally start performing donor area scars in people who intend to keep their hair long, so that any defects in the initial SMP will not be evident to the patient. Long hair masks defects in technique. Scars are a good place to practice in developing the skills necessary to progress to other parts of the scalp. Do not start with a full head SMP or even on a person who shaved his head to show you the scar as you will regret that decision. Make sure you have the technique down before moving beyond donor area scars.
Physician education and training: This has been a real problem as many doctors have accepted tattooist expertise as the authoritative way to approach SMP. Unfortunately, many of these “experts” have produced substandard work (by our standards). Clearly, if they can perform the entire amount of work required in less than half the time as it takes us and in half the number of sessions, what they are doing can’t be an apple-to-apple comparison. Unfortunately, we are repairing many of the patients done elsewhere. We send many of them to a dermatologist that has a Q-switch laser to remove the dots so we can start on a clean slate. The doctor must master the SMP process and this is no different than the doctor who delegates FUE and does not master this procedure.
Cost for SMP: We spend an average of 12 hours on a strip scar in three 4-hour sessions and 20-30 hours for a full head SMP, sometimes with two technicians working on different parts of the scalp. Strip scars require blending in the scalp above and below the scar, so the magnitude of the work increases beyond the strip scar itself. If blending is not done, the scar that received SMP will stand out like a “light bulb.” Pricing, therefore, should reflect the time invested with the patient. For the first session, we usually “undershoot” the final target of what we eventually will do. Session one tells us how the patient’s body reacts to the inks, something about the technique we use and the color we employ, and if the patient’s immune system attacks and removes the inks. We keep careful notes on what we did and how we did it on session one. In session two, we look at the changes that occurred in the results from session one and what we did with regard to color and ink depth. In session two, we repeat the same process, adjusting what we learned from session one, placing the stippled dots directly in the same position as performed the week before, possibly altering the color of the inks and the depth the ink is placed. If the dots are placed too close to other dots, the discrete nature of the stippling may disappear into a confluence of dots that appears blotchy. Good hand-eye coordination is necessary for this. We often determine the final density of the stippled pattern in session two and might adjust the color based upon patient feedback and what we see from the patient’s immune system as it reacted to the ink. Session three is again at least one week from session two and essentially is a repeat of techniques we learned in session two, keeping careful records of what we did, and then we fill in areas that need to be filled, as we refine the overall patterns even further.
By the end of session three, most but not all patients have finished the process. A small handful of patients come back again and again for as many as 7-8 sessions if they continue to attack the inks in their scalp. We lose money on these patients, but the cost of their care is calculated into the overall charge for all patients. If you attempt to try to do the SMP in significantly less time than we take, you will get results that are not comparable to ours. Unfortunately, at this time, there is no short-cut. Any tattooists and other SMP delivery providers claiming that they perform SMP in less than half of the time it takes for us to do SMP, will not get the type of results we see. Side by side, these results will not be comparable to our results.
The authors have previously published SMP for the treatment of a variety of medical and surgical alopecias including scarring from many different causes. In these previous reports, examples of SMP in the treatment of scars have been well documented pictorially, some examples of which are shown in Figures 2-7, and others can be found on our website at https://scalpmicropigment.com/.

Scar before SMP

Scar after SMP

Before (top) and after (bottom) SMP to bad scarring
Before (top) and after (bottom) SMP to donor scar

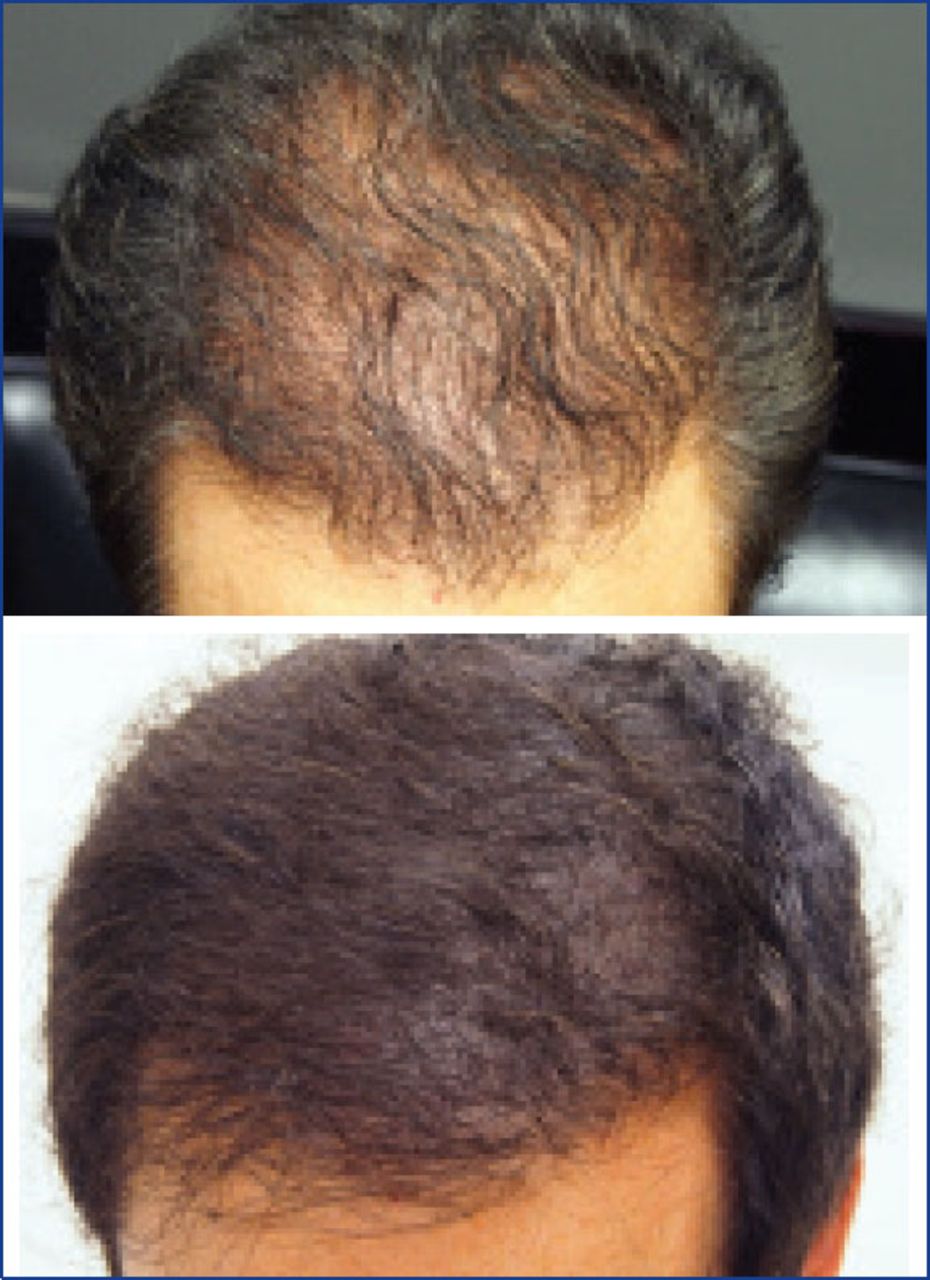
Before (top) and after (bottom) SMP to thinning hair

Before (top) and after (bottom) SMP to beard
Below, Drs. Antonio Ruston and Bessam Farjo were willing to share their personal and professional experience with SMP.
My SMP story—Dr. Antonio Ruston
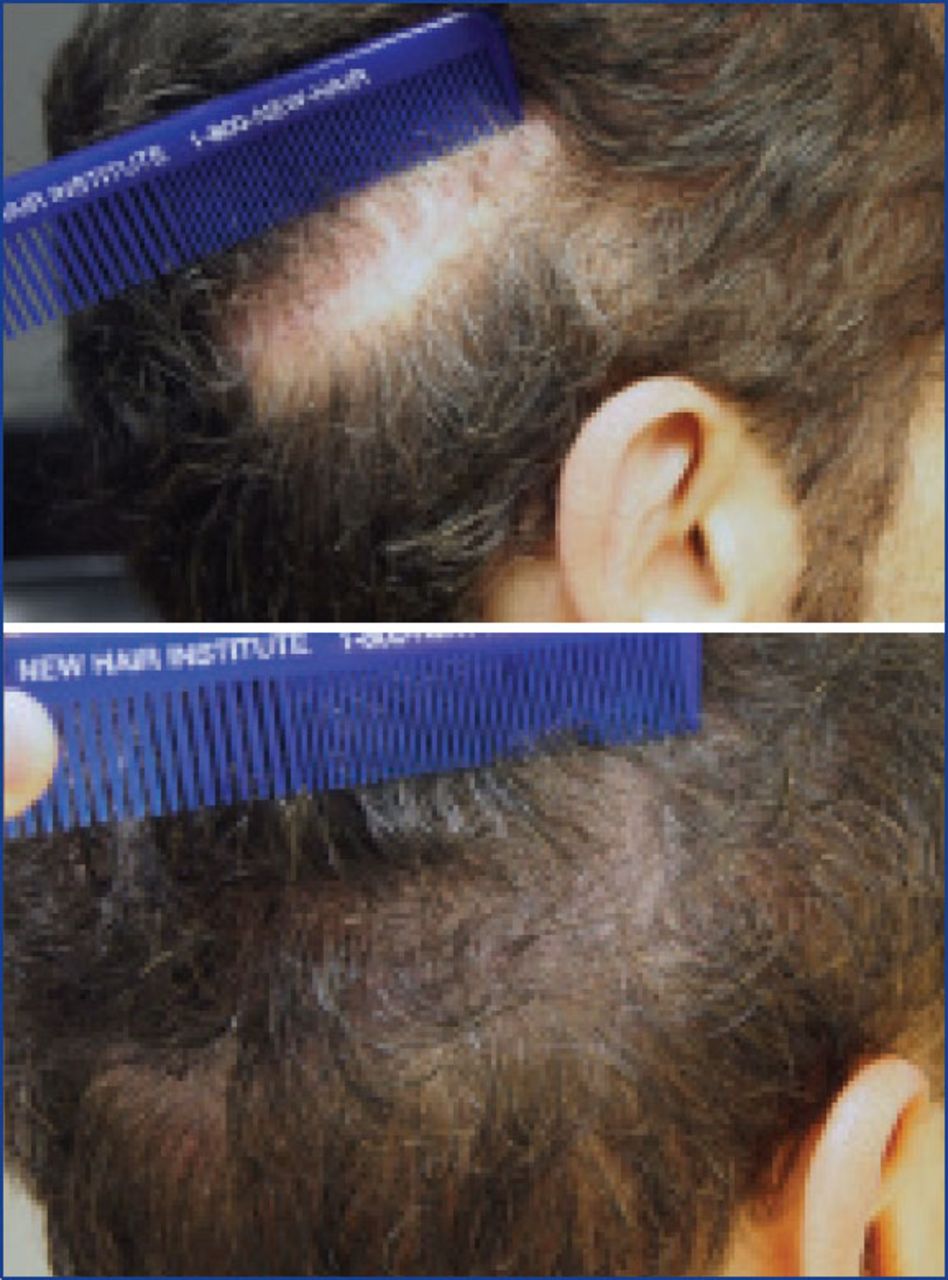
About 25 years ago, I had my first hair transplant to increase the density in the frontal area as the hair had been thinning for some time. The result in terms of density and volume was incredible because large plugs were used and it led me to undergo a second hair transplant 3 years later. However, only when my native hair (not transplanted hair) began to fall out did I realize that my results were very unsatisfactory. I had visible plugs in the transplanted area and a widened scar at the nape of my neck, as well as numerous punch scars of 4mm diameter (Figures 8 and 9).

Scars from pervious surgery

Scars extend to right side
The rest is history.
In the first year of my plastic surgery residency, I decided to study the hair transplant technique and specialize in this field. First, I had to resolve my own problems, and as I learned from actions taken on me, I was able to correct similar cases to mine. So many of these patients received a major aesthetic and psychological benefit from what I learned. Now, 20 years later, I am working exclusively in hair transplant surgery, an interesting evolution in my professional career.
I have had two additional surgeries with the FUT technique to correct my previous surgeries and hairline. One of them was performed by my own team and the other was performed by my friend Dr. Ronald Shapiro, who improved the hairline and did a scar revision to reduce the worst of the scars. Two years ago, I decided to undergo another procedure. This time it was the FUE technique with Dr. Jose Lorenzo, who, with expert skills, extracted follicular units from my scalp and beard, increasing the density in the crown region, and at the same time, he re-created my temporal peaks.
But something was still bothering me as I did not feel liberated. It was the unaesthetic scars in the donor area and nape of my neck that, due to their location at the nape of my neck, could not be hidden. The scars were huge and very visible. What could I do? Extract more hair with FUE to camouflage the scars? Maybe. But what could I do to lower the hairline in the nape of my neck with an already depleted donor supply?
This was when I saw the first SMP case by Drs. Jae Pak and Bill Rassman at our annual congress in Alaska. That was something new for me. A patient with alopecia totalis who, after SMP, appeared to be someone with a full head of hair, but who wore it shaved. I had never seen such perfect work. This patient was the perfect combination of a masterful technique and an art form.
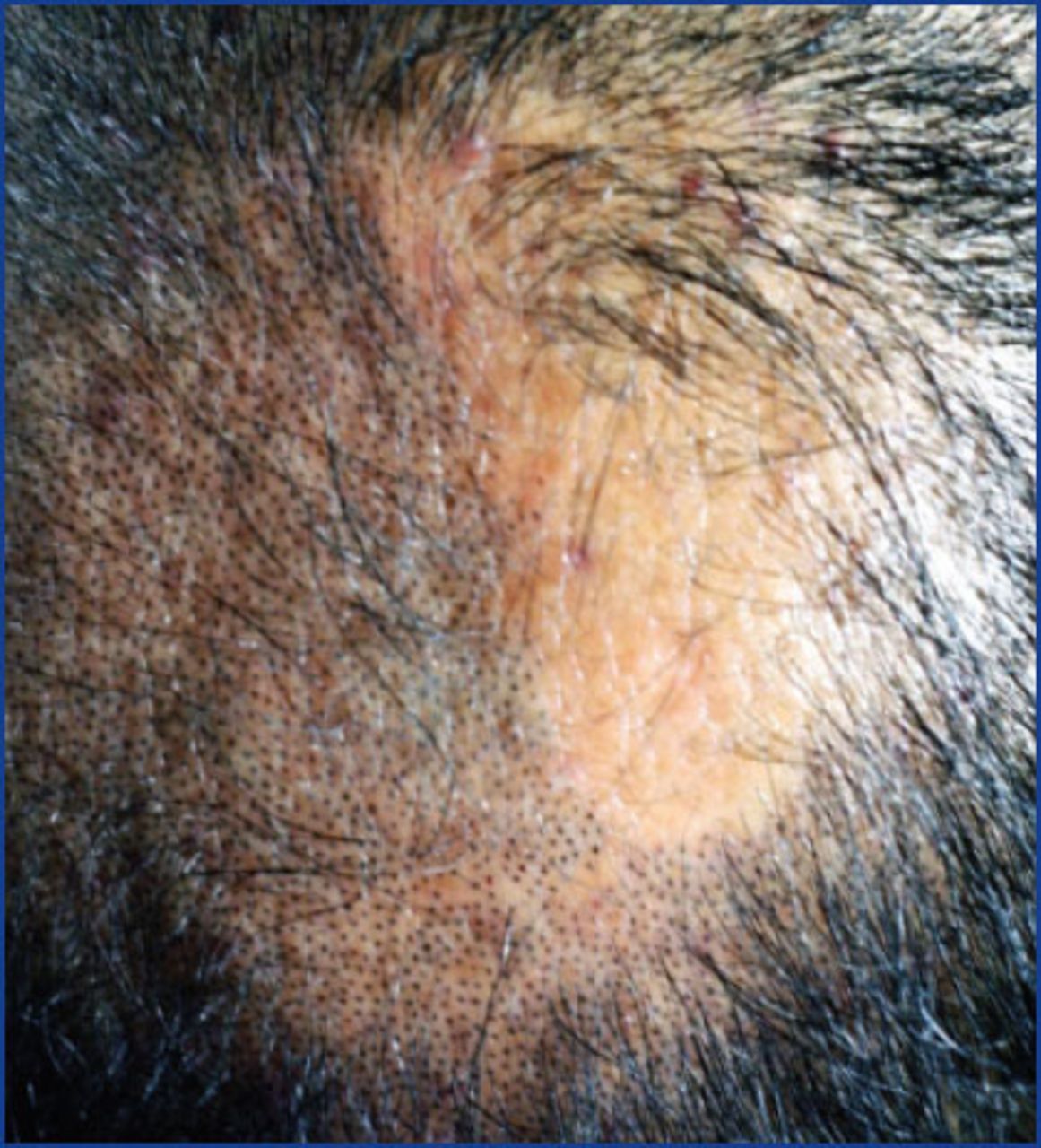
So I bit the bullet and decided to seek out Dr. Pak and bring my scalp to his care. He performed 2 sessions in about 7-8 hours each, where he created what appears to be hair in the nape of my neck. He covered and camouflaged the scars and further addressed all of the other scars on my head and eventually he addressed the FUE punctate scars that came from a FUE megasession (Figure 10). I could not be happier with the result. To give you an idea, I recently participated in a hair transplant workshop, and those who did not know about these procedures and my long arduous history, said to me, “Tony, you decided to wear your hair shaved? It looks great!”

After SMP
I have only Drs. Pak and Rassman to thank for that. The work they perform goes beyond a simple “state of the art” process with SMP. Thank you, Jae and Bill.

FUE and SMP to cover FUT scar.
My experience with SMP in my practice. A very good indication for SMP is when an FUE patient comes with a thick linear scar from previous FUT surgeries. In these cases, they don’t have a real idea about how aesthetic or unaesthetic their scar is because hair was covering the scar. Surgeons see this when they shave the donor area for FUE. Some patients feel uncomfortable with the appearance of the scar and hide out until their donor hair grows to a necessary length to cover these terrible scars. In these cases, we are offering SMP over 2 consecutive days just after the surgery and the following day or possibly one week apart. This way, we can camouflage the scar until the hair grows back and cover it to avoid the problem of a visible scar.
Another indication for SMP is to camouflage the FUE white dots minimizing evidence of extraction in the donor area. We suggest this to the patients when the extractions were excessive or when the white dot scars are more visible with shorter hair styles.
My SMP Story—Dr. Bessam Farjo
How many times do you hear your patients tell you that they have the wrong shape for a shaved head?! Well, I never thought that I would do it, and certainly had no intention of doing so up until about 18 months ago. At the same time, I often regretted having hair transplants too early in my hair career before fully understanding my potential limitations. I thought I needed to practice what I preached.
Around 10-15 years after my first transplant, my donor area began to thin, so much so the multiple donor scars from the strip surgeries of the early 1990s were beginning to show through. This also reflected in the density of the transplanted hair. There was no worthwhile option of further surgery, so the logical thing to do was to resort to a very short haircut. Unfortunately, a point arrived when the donor area was so light that the donor scars were showing with the short haircut.
The initial idea was to apply SMP to the donor scars and the surrounding scalp to act as camouflage so I could maintain very short hair in the donor to counter the imbalance of the hair loss. I used a local and quite confident technician recommended to me. Sadly, the result was unsatisfactory with large, sparse and quite blue dots. I think a number of things were wrong from the inks used right through to the depth and duration of the injections.
This is when I discussed the issue with Dr. Bill Rassman at a meeting and we decided to try their inks and technique. The result throughout the donor area was night and day compared to my previous experience. After a couple of visits, the treatments enabled me to have my hair at the back to only a few millimeters long.
It was that confidence in the quality of the work and the convincing look of the result that encouraged me to have the top and the front of my scalp treated as well during my third and fourth visits. I don’t know how long it will take for the ink to significantly fade but my journey with Jae and Bill started in February 2014 and I’ve not yet had to significantly top up an area (Figures 12-14).
Almost on a daily basis, I take off my surgery hat during a consultation to demonstrate the potential of SMP to a patient who I relate to. They are amazed every time!

Before (left) and after (right) SMP

Before (top) and after (bottom) SMP

close-up of Dr. Farjo’s hairline
Discussion
Scalp micropigmentation uses specialized techniques and conventional tattoo instruments with organic inks in a stippling pattern on the scalp by skilled doctors and technicians trained in the art of the process. The process is very difficult to master because it requires a “feel” using reciprocating needles through the skin. Without a good feel developed, frequent errors occur by those operators inexperienced in the process, often causing disfiguring patterns on the scalp. The problems include amalgams of ink that appear blotchy, inks that do not hold, or color changes in the ink based upon poor ink (pigment) selection.
The process can be used in patients with thinning hair who are not candidates for hair transplantation such as the majority of women with thinning hair (50% of post-menopausal females). Similarly, many men who have received hair transplants and do not get the fullness that they wanted can often obtain their desired end results with SMP. As this is a non-surgical treatment, it is attractive for many patients who find themselves wanting more hair but not wanting to or able to undergo more hair transplants, for whatever reason. The SMP process is a permanent solution to many hair and scalp problems that cannot be treated with traditional hair transplantation, and acts similarly to powdered fibers without the messy problems associated with these products. The SMP market may reflect possibly millions of men and women and patient satisfaction is very high when done well.
Conclusion
SMP offers a good non-surgical adjunctive treatment for solving problems in patients with thinning hair or for those who may not be candidates for hair transplantation and in filling a series of other cosmetic scalp and hair needs. This paper demonstrates the results with the use of tattoo inks in the skin with a stippled pattern. We believe that SMP is destined to become a standardized offering for physicians specializing in cosmetic hair procedures either for primary first use or as a secondary use to augment hair transplantation.
- Copyright © 2016 by The International Society of Hair Restoration Surgery
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.