

Introduction
Hair restoration has presented a long and spectacular evolution since it was first performed in the 19th century with surgical use of scalp flaps until the modern FUE and FUT techniques era. Concerning FUT, Uebel, Limmer, and Bernstein and Rassman contributed enormously to the development of current concepts of this technique in the 1990s.1-3 In 2006, Pitchon created and published the article “Preview Long Hair Transplantation.”4 It was not only a new technique, but a revolutionary and complete methodology representing a declaration of quality and excellence achieved by the art and science of hair transplantation.
Regarding FUE, working in Japan before World War II, Okuda was later considered the pioneer of punch hair grafting.5,6 In 2002, Rassman and Bernstein were the first to describe FUE as a surgical technique in medical literature.7 Later, Harris8,9 and Cole10,11 developed a wide variety of devices, punches, and extraction methods that contributed to current concepts surrounding the FUE technique; for example, the FUE procedure does not produce a linear donor area scar, it causes less post-operative pain, it has resulted in the feasible transplantation of body hair to scalp, and it can be performed even in the absence of good scalp laxity.
However, there are also some disadvantages to the FUE technique: it demands a relatively long learning curve and it typically requires patients’ hair to be shaved. The requirement to have their hair shaved is frequently the main objection that makes patients unwilling to undergo an FUE procedure. Hair trimming for FUE and subsequent exposure of a linear scar is certainly considered an issue for patients who have undergone an FUT procedure in the past. The large number of patients requesting the non-shaven FUE technique in Brazil, a country in which FUT is by far more popular than FUE, was the main motivation behind my desire to perform and improve non-shaven FUE.
While doing direct non-shaven FUE, a modality in which the punch cuts skin and hair shafts simultaneously, I realized that using an oscillatory instead of a rotational punch movement was the most effective way for punching, because rotational movement often caused the hair to wrap around the punch. In a search of a method for harvesting grafts with intact hair shafts while performing oscillatory punch movements, I developed the concept of an “open punch.” It makes possible harvesting intact long hair grafts by associating the basic principles of the “preview long hair” concept created by Dr. Pitchon and the FUE technique.
The Open Punch
This new kind of sharp punch has a slit that accommodates the long hair shaft inside the punch while the graft is being punched with an oscillatory movement. This slit may vary in length and width according to skin/hair type and whether the surgeon is using a manual or motorized device. One interesting aspect is that the slit allows the surgeon to have a good view of the emerging hair, facilitating an accurate insertion angle (Figure 1).
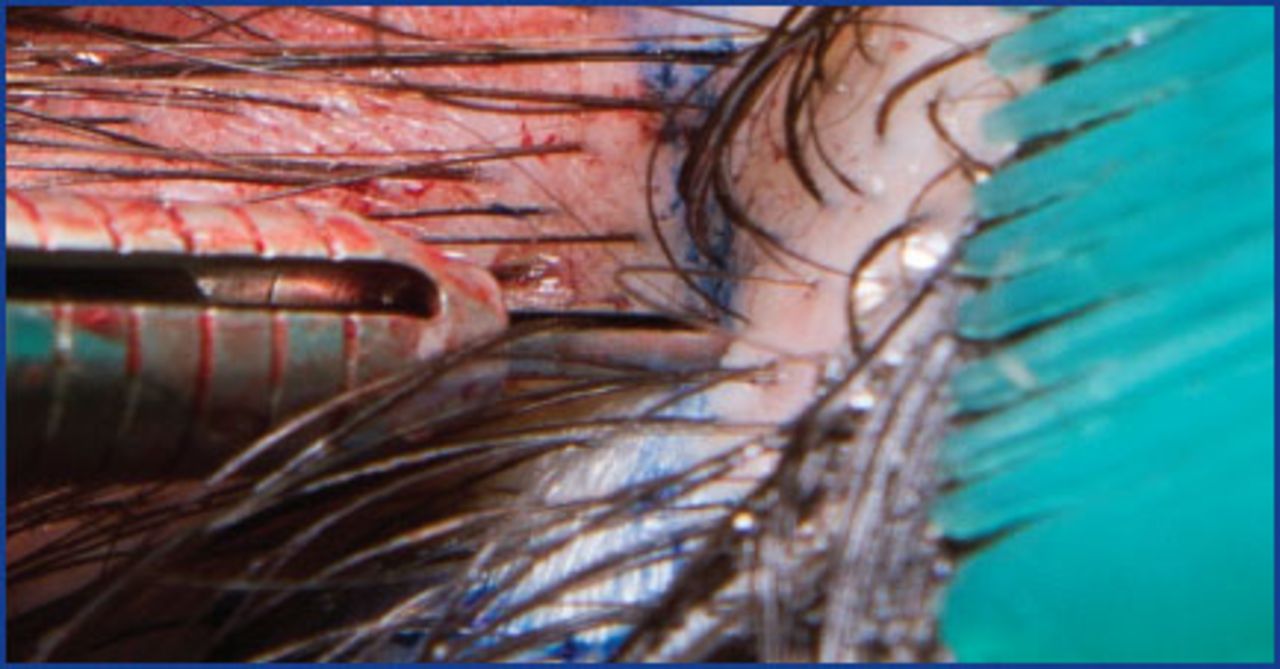
The open punch aligned with long hair
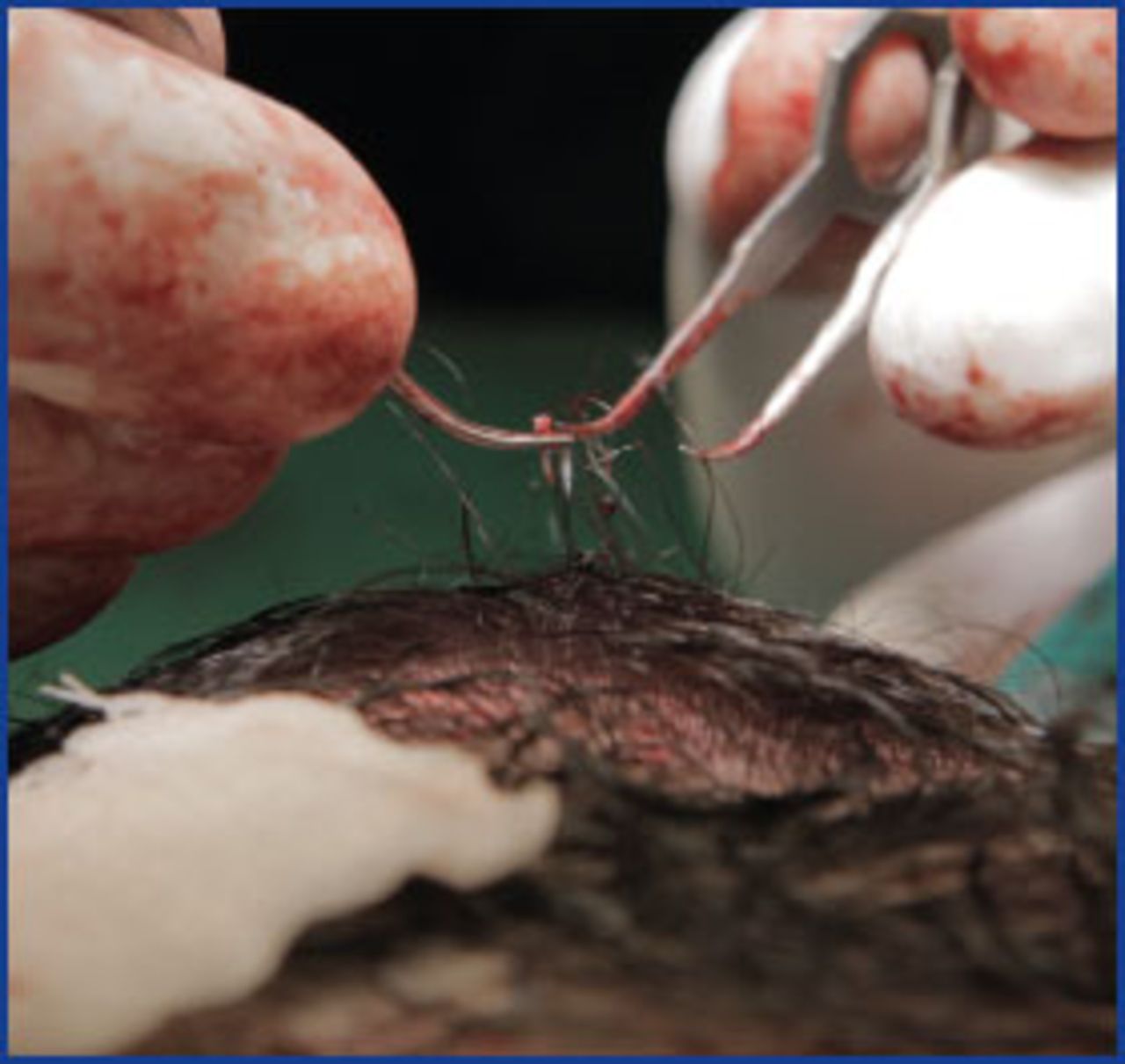
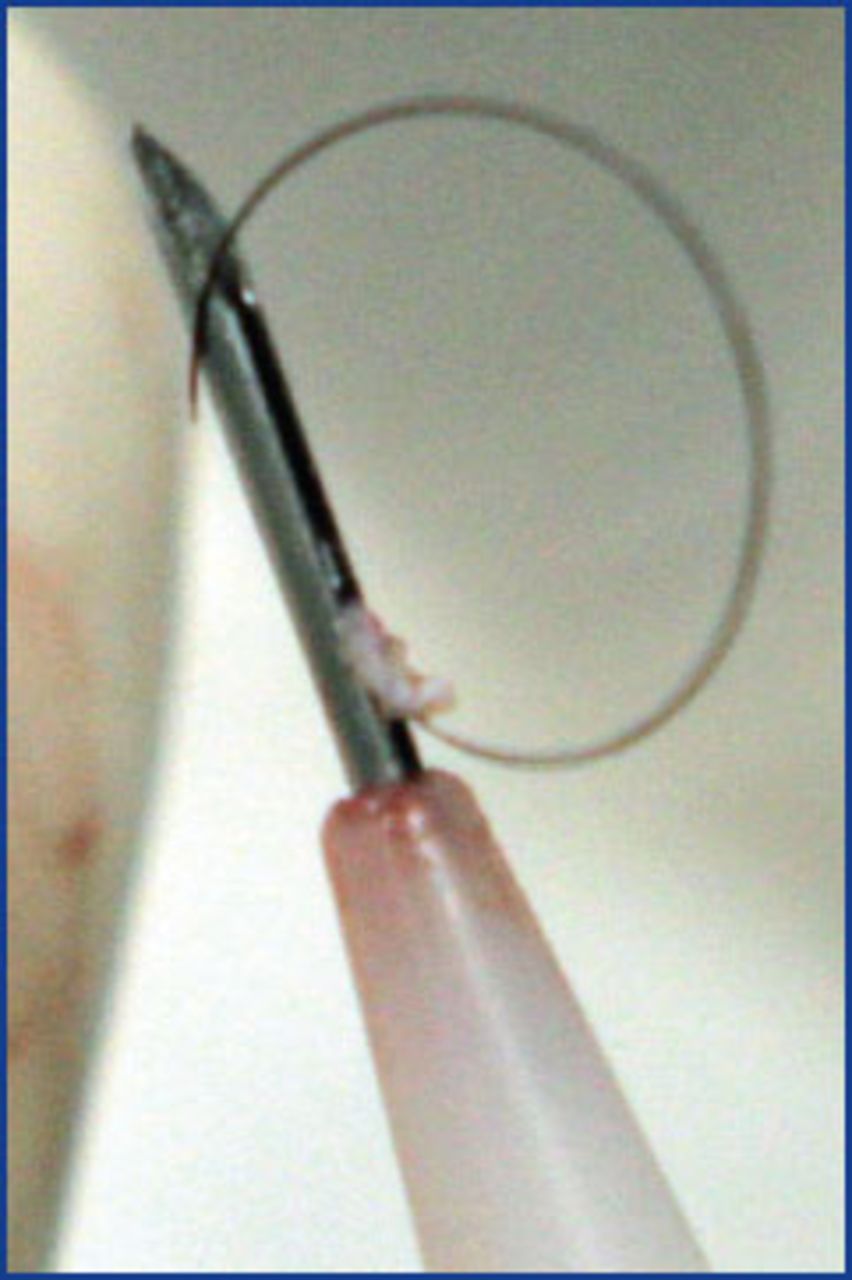
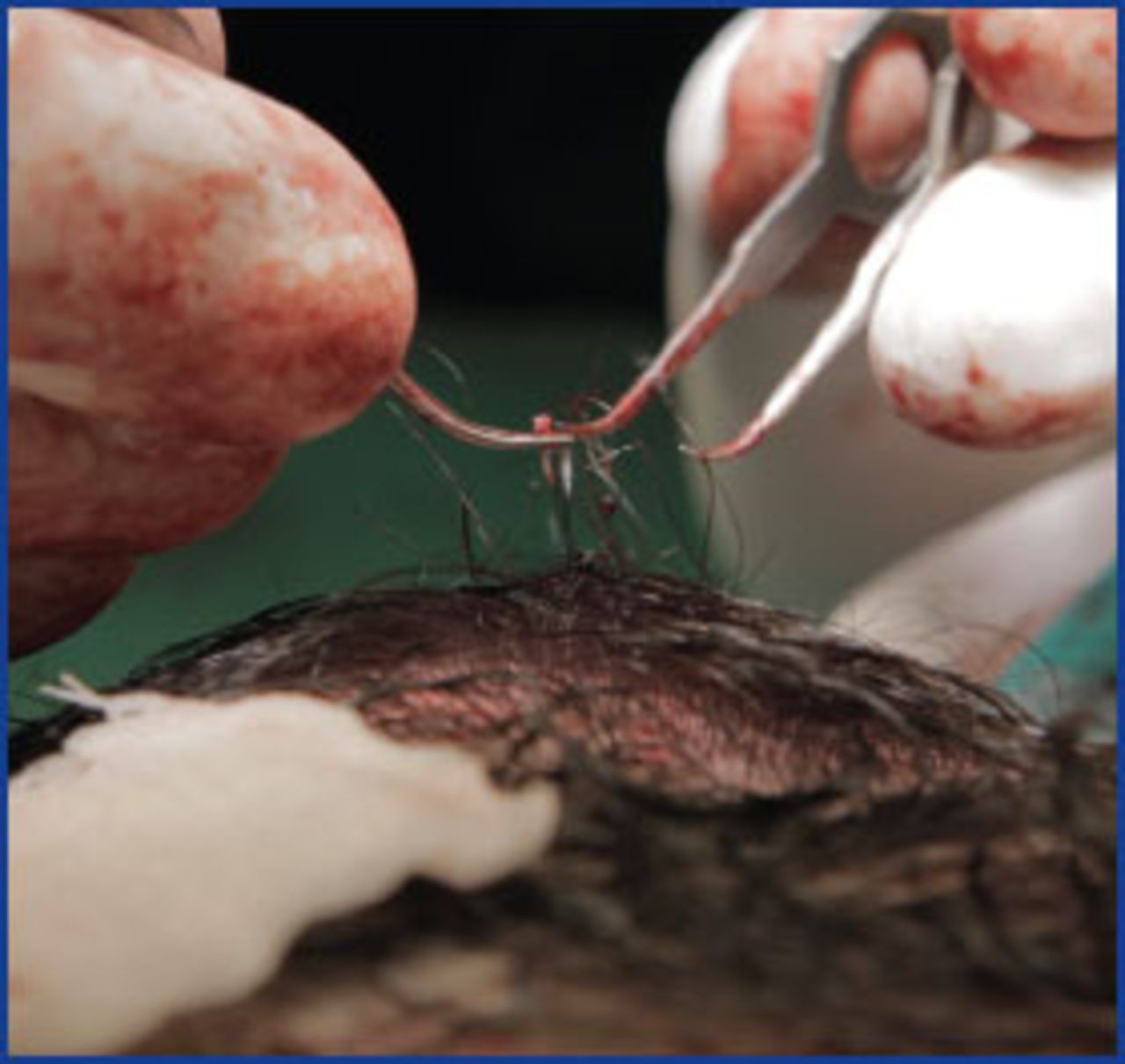
I tested a variety of punches with slits of different shapes, depths, and widths. By increasing slit width, I found I could easily align the hair shaft with the slit, however, there was more capping and the manual extraction was harder. When I reduced the slit width, it was harder to place the hair in the punch but, on the other hand, it reduced capping. Capping in this case happens as a result of too shallow insertion depth, but also due to incomplete cutting of the epidermis around the graft. I found the best compromise to be a larger slit width combined with a larger oscillation arc. My first punch design had a 0.25mm slit width, a 4mm slit depth, and a 1mm punch diameter, and sharp edges (Figure 2). I chose a 4mm slit depth because the punch rarely needs to reach a depth of 3mm or more to allow graft harvesting. It was easy to place the hair shaft in the punch with a 0.25mm slit width, but difficult to perform manual extraction. However, with a 0.25mm slit width and a motorized oscillation set as high as 420, grafts were easily extracted. To reiterate, with the manual FUE device, most of the time, after punching, some amount of uncut skin remained around hair shafts, producing capping (Figure 3) and making graft harvesting difficult.

The first project of the open punch—designed with 0.25mm slit width and 4mm slit depth
Note epidermis around the hairs producing capping after punching with the open punch with 0.25mm slit width.
After some further adjustments, I finally settled on a 0.125mm slit width and a 4.5mm slit depth, with 1 and 0.9mm punch diameters. This reduction made hair insertion in the punch harder, but the capping issue was eliminated, manual extraction became feasible, and motorized extraction with oscillation arcs of 270° to 360° worked very well (Figure 4).
Perfect long hair FUE graft just after harvesting.
Harvesting Technique
I recommend dividing the donor area into boxes. This makes it possible to perform a more homogenous extraction, especially with long hairs in the donor area. Also, follicular units in the same regions usually present similar emerging angles, directions, and depth. When moving extraction to other squares, all parameters, mainly the depth control, must be checked again. Local anaesthesia and tumescence must be done as the surgeon routinely performs on shaven FUE.
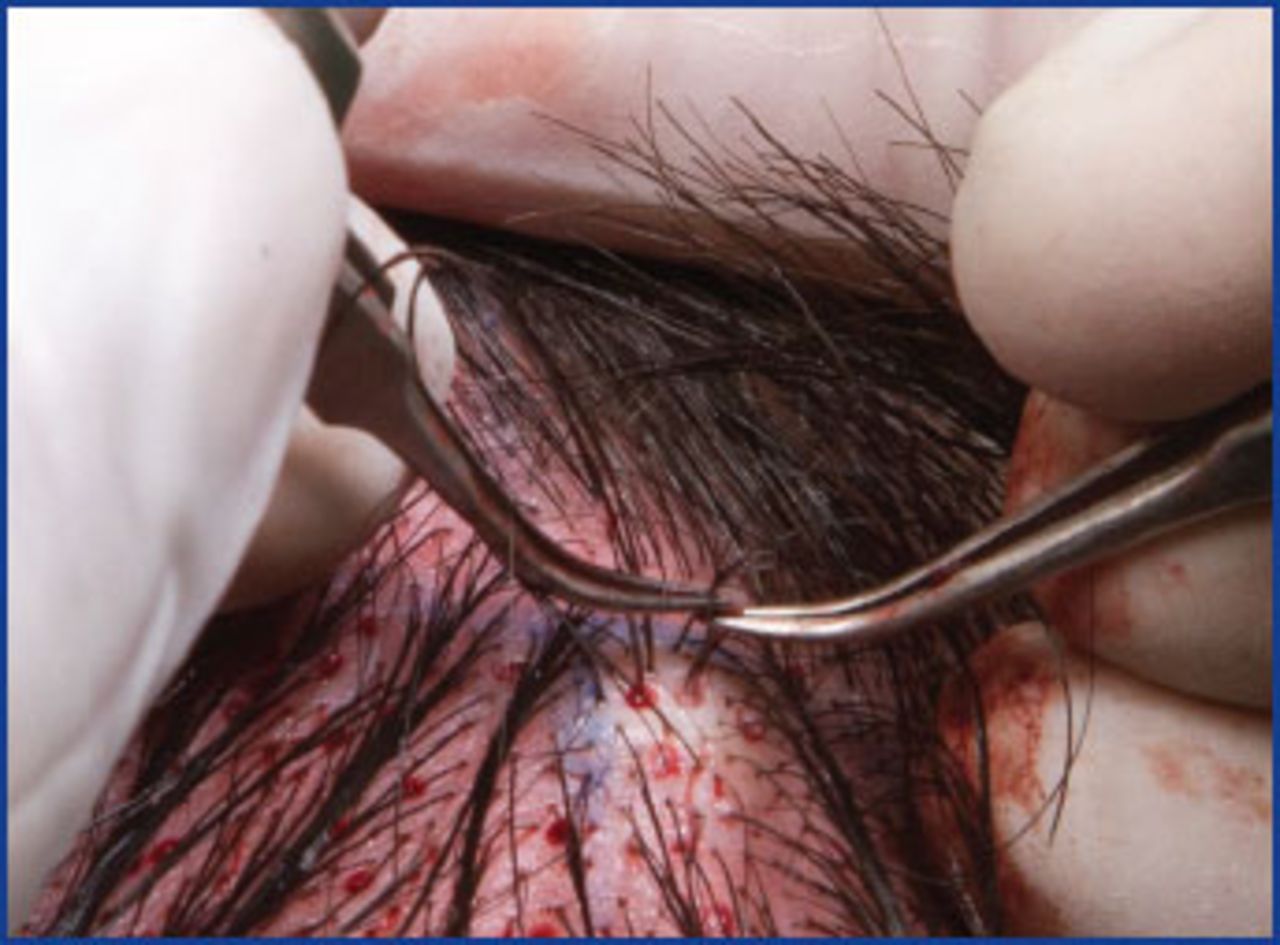
Two kinds of combs are used in order to manipulate hairs. A surgical assistant uses one regular comb to hold the long hairs in the upright position. The surgeon uses a modified “mini-comb” to move the hairs up and down during extraction (Figure 5).

Improvised mini-comb (pink)
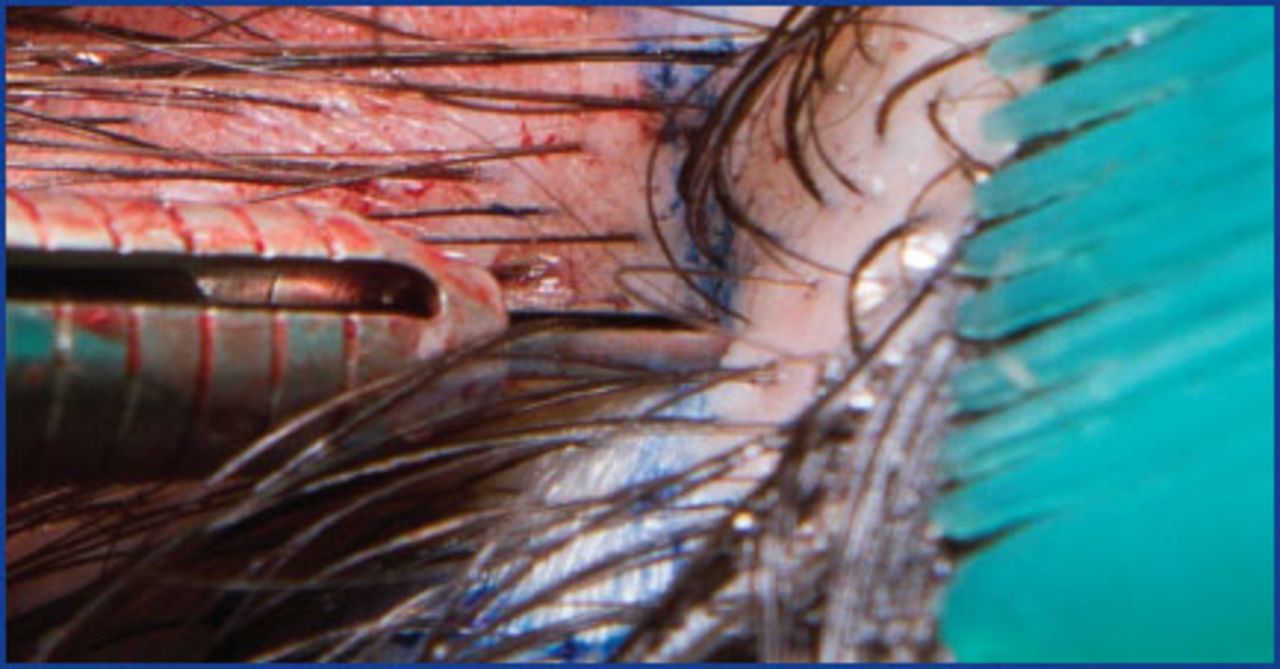
The initial step is to align the punch and the long hair of the targeted follicular unit at a correct angle (Figure 1). The punch cutting surface must completely touch the surrounding skin and then the punch oscillated in a 270° to 420° arc. The surgeon must also adjust punch depth as is routine in all FUE. Regular forceps or ATOE are used for graft removal.
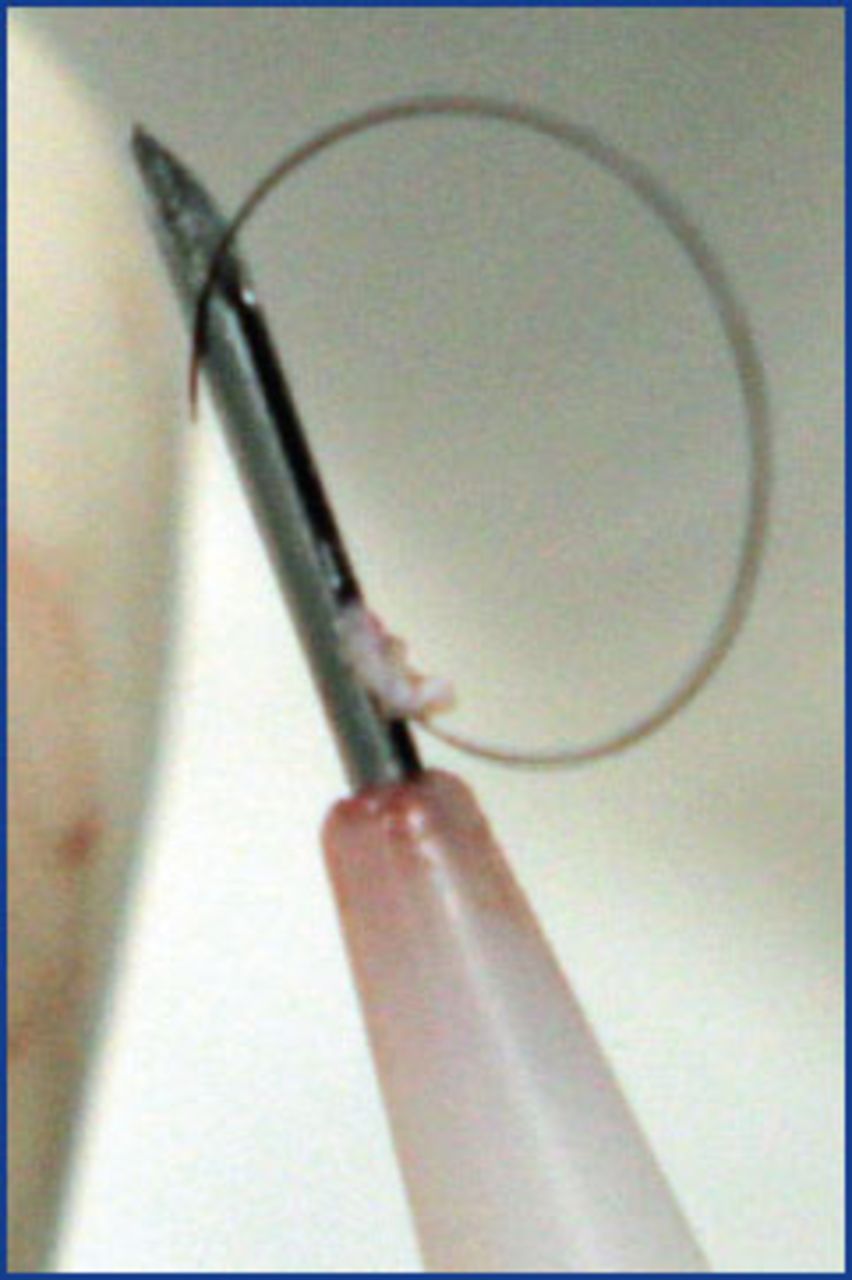
For placing FUE long hair grafts, I prefer implanters once hair curvature control can be easily achieved while loading. I position the convexity of hair curve toward the needle axis (Figure 6). This way, the hair angle can be oriented correctly while placing.
Loading the implanter. Note hair convexity facing needle axis.
Case Study
The patient was a 36-year-old male with a traumatic alopecia on the right temple due to a previous neurosurgery, with consequent craniotomy scar reaching temple parietal and occipital areas. His goal was to cover the scar surface on the temple area, but, at same time, he did not want to get another linear scar on his scalp. This surgery took 5 hours and used 549 grafts (134 singles, 232 doubles, 183 triples) (Figures 7-10).
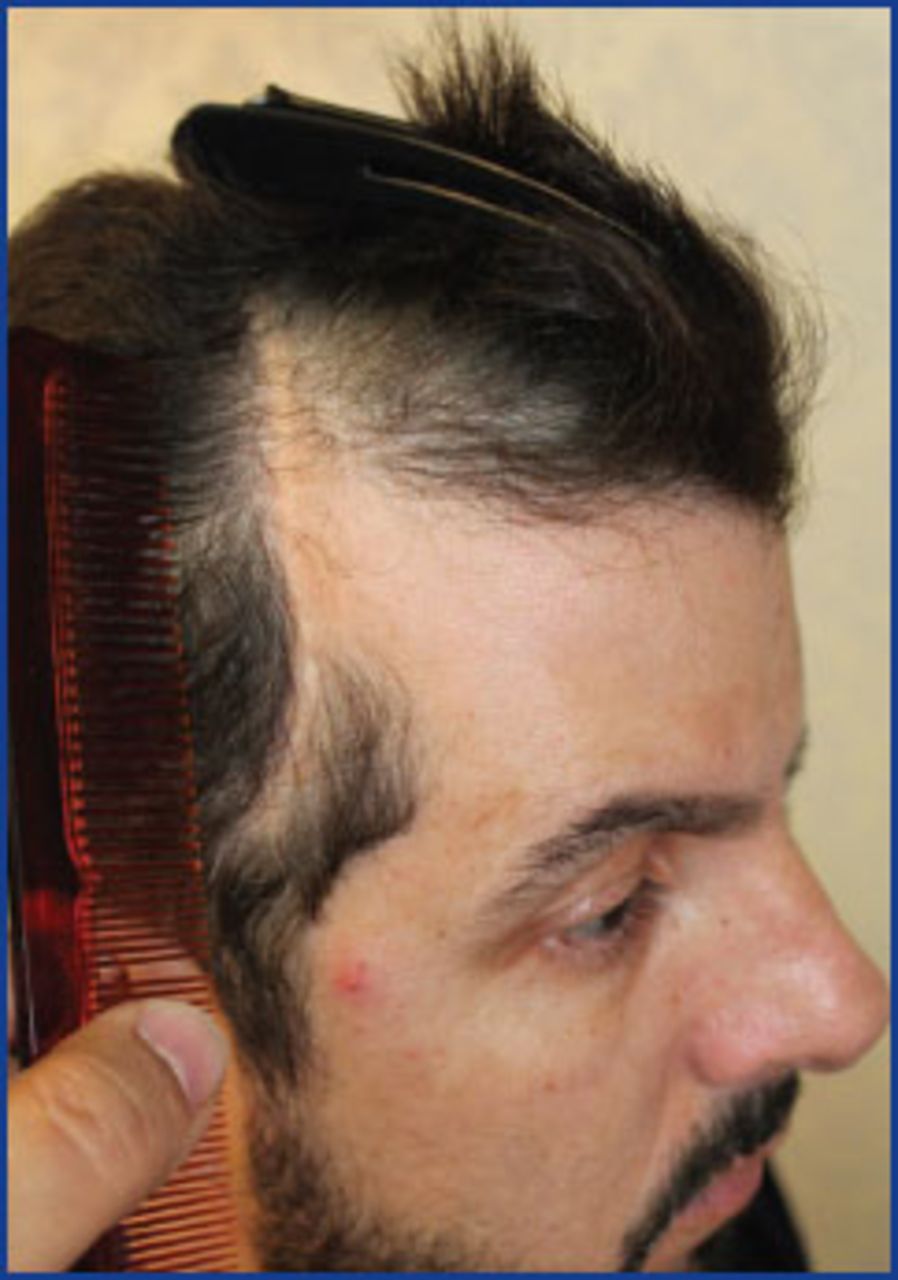
Pre-operative view

Defining recipient area

Seven days post-surgery. Note aspects in donor and recipient area.

Close-up view of recipient area at 7 days post-surgery
While performing long hair transplantation in this case, I could extract the exact number of follicular units required to cover the scar surface, allowing perfect hair angle positioning on the temple and temple peak area. There were 1,314 hairs extracted; of these, 167 were transected, for a 12.7% transection rate. I used a 1mm open punch and harvested 300 grafts per hour, contrasting to 800-1,000 per hour I usually achieve when I perform regular shaven FUE cases. Placing grafts in this case took longer due to the large scar surface with hardened skin of the patient’s recipient area. To watch a video of the technique, go to https://youtu.be/NeLmtrQB9RE.
Discussion
Pitchon established during his studies the “Personal Growth Index,” or “PGI,” which refers to the percentage of transplanted hair that has actually grown when outcome is complete and definitive.12 He defined “Delta Loss Index” as the approximate percentage of hairs that did not grow. He created these indicies when assaying hair density differences between the provisory or immediate post-operative period and the definitive outcome months later.
Trying to adapt the PGI and Delta Loss Index to long hair FUE, I faced a new dilemma: to cut or not to cut transected, bulbless hairs from follicular units? This concern was based on hair regeneration knowledge—hair shafts with no bulb usually but not always do not regrow.13,14 Keeping these bulbless hairs in the grafts may give a false impression to the patients with long hair preview. Thus, patients must be made well informed about this concept during their preparation for surgery. In order to compensate, the surgeon can implant a small percentage of short hair grafts that do not add visible density to the preview result.12
Another interesting concept regarding preview long hair that may be very useful in long hair FUE is the “density selection reverse.” With preview, we first cover the recipient area and then we determine what the necessary density to achieve a proper coverage is. While performing shaven hair transplantation, density is defined first and only some months later will we find out what level of coverage we have achieved. The density selection reverse concept allows surgeons to achieve the necessary cosmetic coverage with the minimum number of follicular units, minimum surgical aggressiveness, and minimum morbidity. Besides all known advantages of preview long hair, such as hair angle control, crusts and erythema camouflage, and immediate visualization of result with instantaneous emotional reaction from the patient, the long hair FUE technique also allows the surgeon a precise control of how much to harvest from the donor area, avoiding overharvesting. I have termed this new and interesting concept regarding long hair FUE “donor area preview.”
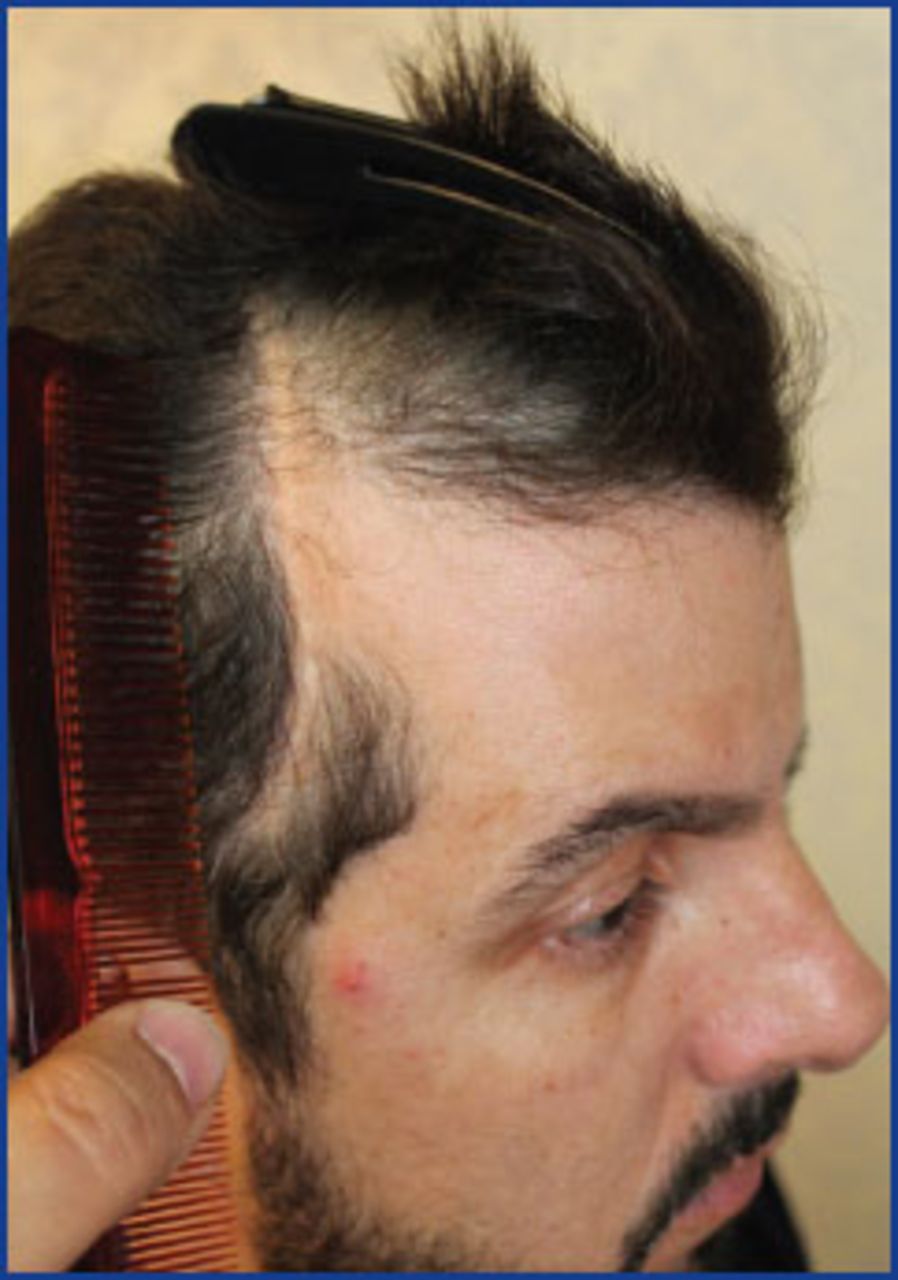
While performing long hair FUE, the surgeon can appreciate seeing a progressive hair density reduction on donor area during the harvesting process. This is very important for patients with intermediate or low hair donor density, especially if they have undergone previous strip procedures, as the 35-year-old patient shown in Figures 11 and 12. He had two strip scars, poor laxity, extensive bald area, and intermediate donor area hair density. In such cases, the amount of hair presented by the patient may be insufficient to cover a large bald area and to totally camouflage the previous strip scar.

Extensive bald area Norwood-Hamilton grade V

Two previous strip procedures, large linear scar, very poor laxity, intermediate donor area hair density
A good option in cases like that, in my opinion, besides scalp micro-pigmentation to the strip scar prior to surgery, is carefully performed long hair FUE in which the extent of harvesting would be controlled by utilizing the density selection reverse and donor area preview concepts. Thus, the surgeon will achieve some coverage with the minimum use of follicular units, and at same time will balance the reduction of donor area hair density. By following this approach it is possible to identify when to stop harvesting in the interest of the appearance of the donor area.
A disadvantage of the open punch is the impossibility of using full punch rotation. Oscillatory movement is essential for manual or motorized long hair harvesting. Using 5-6× magnification loupes is very helpful during long hair FUE especially for inserting the long hair shaft into the punch.
Long hair transplantation seems to be fundamental in areas where hair angles must be very precise, as in eyebrow transplantation. Long hair FUE also may be useful in cases when preview long hair FUT is limited by poor laxity or when the surgeon needs to harvest additional grafts complementing a traditional preview long hair FUT procedure, this way performing a combined FUT/FUE technique. For patients who may need more than 1,000 long hair FUE grafts, it is highly recommended performing the procedure in two or more days since this technique is more physically demanding and time consuming as well.
The open punch is transparent in the sense that the targeted emerging hair is visible inside of it. This facilitates aligning the punch according to hair angle and direction. This fact may expand the use of open punch beyond the long hair FUE—it may be very useful for beginners while performing even traditional shaven FUE. My next studies will investigate whether transection rates performing traditional shaven FUE would be somehow affected by using the open punch instead of regular punches. It is justified by the theory that the open punch has a reduced cutting surface—270° to 315°—in comparison to traditional 360° punches. It may improve transection rates in difficult cases such as with curly hair patients.
- Copyright © 2016 by The International Society of Hair Restoration Surgery
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.