

ABSTRACT
The presence of beards in men has intrigued humans throughout history, drawing interest from various fields. This article proposes a universal morphological classification for the human beard, aiding comparative studies and medical communication.
Evaluation of hair and beard transplant patients was conducted on 250 males at the Speranzini Clinic over three years. Types of beard presentation were categorized based on morphological features. The classification was progressive from type I to VI. In our sample, the most frequent beard pattern was type V (42.4%, n = 106), with a mean age of 41 (range 21-66 years old).
The proposed classification offers a standardized approach for beard evaluation across diverse populations. Further research is warranted to validate the findings in different groups. Despite potential ambiguities, the classification was efficiently applied in the studied population.
INTRODUCTION
The presence of facial hair in men has long been a topic of fascination, stimulating interest across diverse realms of human inquiry. A marked reduction in overall body hair distinguishes Homo sapiens from other anthropoids.1 Unlike other non-human primates, humans differ by the absence of fur and a lack of hair coloration regional patterning.2 Within the evolutionary context, sexual selection offers an alternative framework to natural selection for examining the development of facial hair in men. Intrasexual selection among males favors the emergence of sexually dimorphic traits that enhance or signal competitive prowess.1 Beards contribute to perceptions of male masculinity, social maturity, confidence, aggression, and age. While these attributes are valued by females in potential mates, investigations into the relationship between facial hair and male facial attractiveness have yielded conflicting findings.1,3-5
During prenatal development, the fetus is covered in primary lanugo hairs, which are subsequently replaced by secondary vellus hairs during early post-natal life. Throughout infancy, childhood, and adolescence, vellus hairs differentiate into tertiary terminal hairs in specific body regions, primarily under the influence of androgens, although no additional follicles are formed. Beard growth undergoes significant expansion during puberty, continuing until the mid-30s.1,2,6-8
Morphological disparities have been identified between beard and scalp hair, encompassing variations in cross-sectional area, shape, number of cuticle layers, cuticular pattern, and medullation. Facial hair fibers display greater irregularity in shape compared to scalp fibers, with nearly double the number of cuticle layers. Furthermore, cross-sectional area for beard hair has been observed to be 70-100% larger than that of corresponding scalp fibers.2,9,10 Minor variations in fiber size, geometry, and pigmentation are influenced by ethnic origin.9 Additionally, different ethnic groups exhibit variations in the pattern, distribution, and density of beard and body hair. Indians, Middle Easterners, and Caucasians typically exhibit higher hair density in their beards and mustaches compared to individuals of Oriental descent.1,5,11
Given the multifaceted importance of facial hair in men, this article proposes a universal morphological classification system for human beards, aiming to facilitate comparative studies of facial hair across different populations, aid in the understanding of patients considering beard transplantation regarding achievable outcomes, and standardize medical communication on the subject. Several morphological classifications have been established in clinical practice across various specialties, such as the Fitzpatrick, Tanner, and Capurro Scales.12-14 In the field of hair restoration, decades-old scales, such as the Norwood-Hamilton and the Ludwig scales, remain widely used in clinical practice to this day.15-17 Anatomic distribution patterns of pubic and thoracic hair have also been outlined.18-20 All these classifications are easily applicable in clinical practice as they consider morphological criteria easily defined to categorize populations into different groups, based primarily on characteristics discernible through simple visual inspection.
Anatomic divisions of the beard have been described for the purpose of surgical reconstruction,21 as well as important anatomical lines and points for proper beard design on the face.22 However, to the authors’ knowledge, there is currently no universal classification for the presence of beard hair in adult men. Thus, we describe a progressive morphological classification for evaluating beard hair presentation patterns in men.
MATERIALS & METHODS
We assessed a sample of 250 males who were seen at the Speranzini Clinic over a period of three years; this consisted of 223 patients seeking hair transplantation (89.2%), 19 patients seeking beard transplantation (7.6%), and 8 patients seeking both treatments (3.2%). The mean age was 41 (range 21-66 years old), with most patients between the ages of 40-49 years (35.6%) and 30-39 years (33.2%). Patients who had completely shaved their beards at the time of consultation, those who had undergone laser hair removal on the face, individuals with cicatricial alopecia, and those with sequelae of traumas or previous surgeries in the facial region were excluded from this study.
Following a thorough physical examination, photographs were taken of the anterior-posterior, right lateral, and left lateral views, and these pictures were used to evaluate, identify, and classify facial hair growth patterns. The frequency of occurrence of different patterns was recorded, and the types found were objectively described considering morphological characteristics that are easily appreciated.
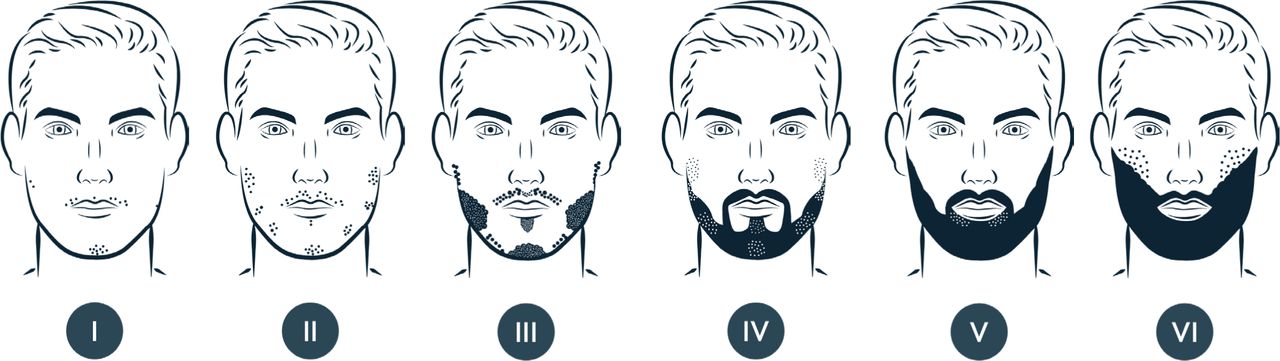
The classification was progressive, so that each described type has more hair and greater coverage than the previous category. The following are descriptions of the types of beard hair presentation that we found:
Type I: Practically hairless. There are a few hairs in small quantities, mainly in the central region of the face, mustache, and chin. Typically, there is no goatee fully formed, but some patients may exhibit few hairs between these regions. Some anatomical regions of the beard do not present any hair at all.
Type II: Presence of hair in the central region of the face (mustache and chin), but other topographical regions of the beard are already easily identified, albeit with low density, isolated, and with little to no connection. The mustache is thin and is divided into two parts with few hairs in the middle region. Typically, there is no goatee fully formed, but some patients may exhibit few hairs between the mustache and chin.
Type III: Presence of hair in all anatomical regions of the beard, with low to medium density. The mustache is thin and is divided into two parts with few hairs in the middle region. Typically, there is no goatee fully formed, but some patients may exhibit few hairs between the mustache and chin.
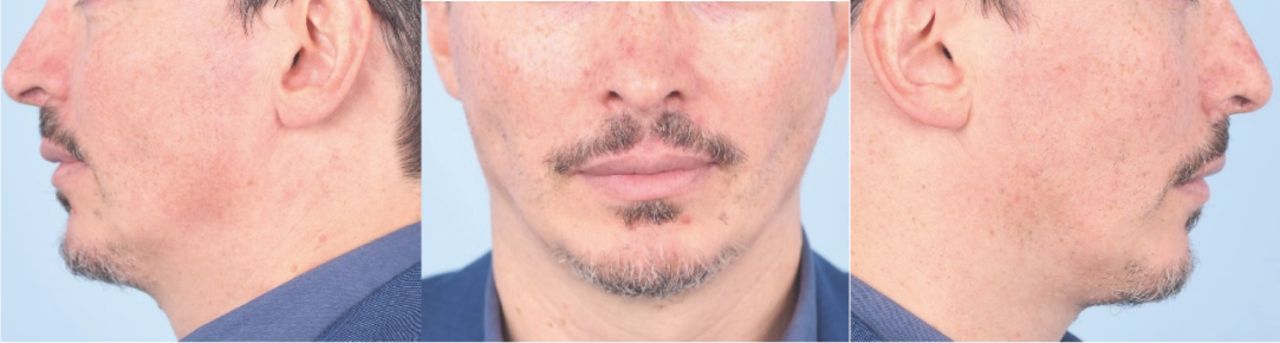
Type IV: Presence of hair in all anatomical regions of the beard; however, at least one anatomical region exhibits much lower density than the others, generally the sideburn or the chin region. Typically, the goatee is fully formed, but some patients may still exhibit separation of chin and mustache.
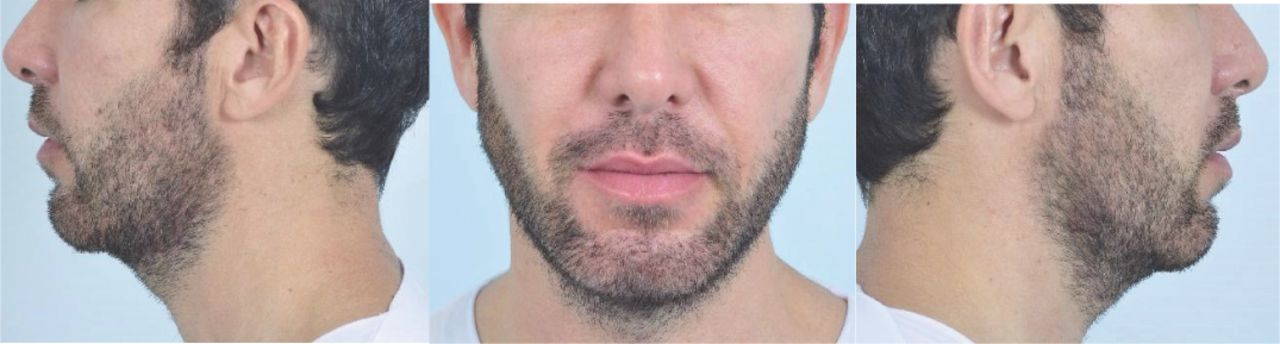
Type V: Presence of hair in all anatomical regions of the beard, with medium to high density. The mustache is generally not contiguous with the maxillary region, leaving an area of recess without hair between these two regions. In the infra-labial region, there is still a persistently low-density area laterally, between the lip and the chin region.
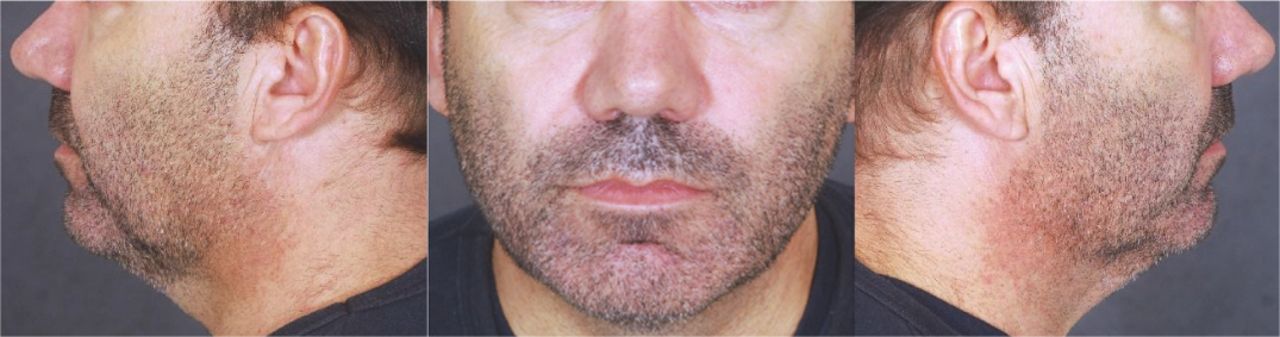
Type VI: Presence of hair in all anatomical regions of the beard, with medium to high density. Some beard hairs extend almost to the zygomatic region, and the mustache does not show disconnection with the maxillary region. In some patients, there may still be a persistently low-density area laterally, between the lip and the chin region.
Tables 1 and 2 show the prevalence of the various types in the studied population. Table 3 summarizes the characteristics by beard type, detailing the presence of hair in each anatomical region. In Figures 1 to 7, we present photographs and schematic drawings illustrating the various beard types.
Beard Types in the Studied Group
Beard Type Distribution by Age Group
Comparison of Beard Presentation Type and Its Characteristics

Beard type I

Beard type II

Beard type III

Beard type IV

Beard type V

Beard type VI

Schematic drawings illustrating beard types I-VI.
Observations
In our sample, we found a few cases of underdeveloped beards in which the predominance of hair in the peripheral region of the face was greater than in the central region (with an almost absent moustache). We consider this presentation a variation of the norm and classify it as type III with peripheral pattern (Figure 8).

Type III peripheral pattern facial beard, with low-density hair in all anatomical regions with the mustache and central sublabial region having the lowest density (this mustache has approximately 106 single hair follicular units) (left); schematic drawing (right).
Regarding the distribution of hair in the cervical region, we observed that it follows a pattern of greater coverage in the central compartment, mainly in the suprahyoid region, subsequently progressing to the lateral regions and inferiorly over the thyroid cartilage. In some patients, there is a persistent gap in the submandibular cervical region, leaving the central and lateral regions separated.
DISCUSSION
Brazil has a highly diverse genetic pool (largely Amerindian, African, and European),23 enabling a wide variety of phenotypic presentations of the beard. Some studies show associations of nucleotide alterations in specific genes linked to the presentation of beard, eyebrow, and hair characteristics in genetically diverse populations (beard-linked gene markers EDAR, LNX1, PREP, FOXP2).2,24 Building on this, several authors have previously documented beard density in its various anatomical regions, though their studies were conducted on small populations and lacked correlation with the characteristics of beard presentation on the face.11,16,21,25,26 We identified a gap in standardizing facial hair presentation that should be helpful to compare different ethnic groups as well as to document the frequency of each described type within each of the different population groups and correlate it with density and genetic characteristics.
Our findings are consistent with the observation that men primarily seek substantial coverage in the central region of the face (mustache and goatee) when undergoing beard reconstruction surgery via hair transplant.27,28 This region is where hair begins to appear during the sexual maturation of boys and is typically the most visible in frontal view. Its absence often draws significant attention, stigmatizing the hairless man, which may lead to psychological trauma by associating him with low sexual development.8
A progressive classification can also aid in aligning the expectations of patients seeking hair transplant surgery for beard enhancement, often with unrealistic expectations of achieving a complete and densely populated beard in a single procedure, with minimal use of donor area on the scalp or neck. With this classification, we can predict the follicular unit (FU) requirement for a patient to progress from one grade to another on the scale, and whether this “progression” is achievable through surgery. For instance, a type I patient will not be able to progress to type V or VI, except with the use of an exceptionally large number of FUs from the scalp; thus, it is prudent to conserve donor area and transition to a type III or IV. Illustrative photos can serve as examples for patients of how a less dense beard can still be aesthetically suitable.
The ease of patient classification is also noteworthy. No calculations, devices, or exams are required. Just a quick visual inspection suffices. This classification does not consider the length of beard hair, as it is known that hair length is an important factor in determining hair volume29 and may give a false impression of hair distribution completeness. Even with a short beard, we can accurately classify the patient’s type based on the presence or absence of hair in the topographical regions of the beard. However, in patients with freshly shaved beards, it is not possible to classify.
A caveat that needs to be made concerns the sample studied. Our sample included, albeit in a small percentage, patients under 30 years old (10.4%, n = 26), which may lead to an inadequate assessment of the actual development of the beard due to their young age. In practice, we observe that patients with sparse beards seek improvement through hair transplant surgery at a very early age. Within the 20-29 age group, there is proportionally higher demand for beard treatment compared to other age groups (23.1% of patients seek this treatment, compared to the overall average of 7.6%). Generally, there is a decrease in the search for beard treatment as age advances. In the sample, this pattern is only broken in the 60-69 age group (10% seek beard treatment). However, the sample size in this group is smaller, having only 10 patients, which may make the set more susceptible to fluctuations. Table 4 shows the cross-tabulation between age group and treatment with distribution of treatments by age group and percentages in the rows.
Cross-tabulation between Age Group and Treatment Appointment (Beard Surgery, Hair Surgery, or Both) with Distributions of Treatments by Age Group and Percentages
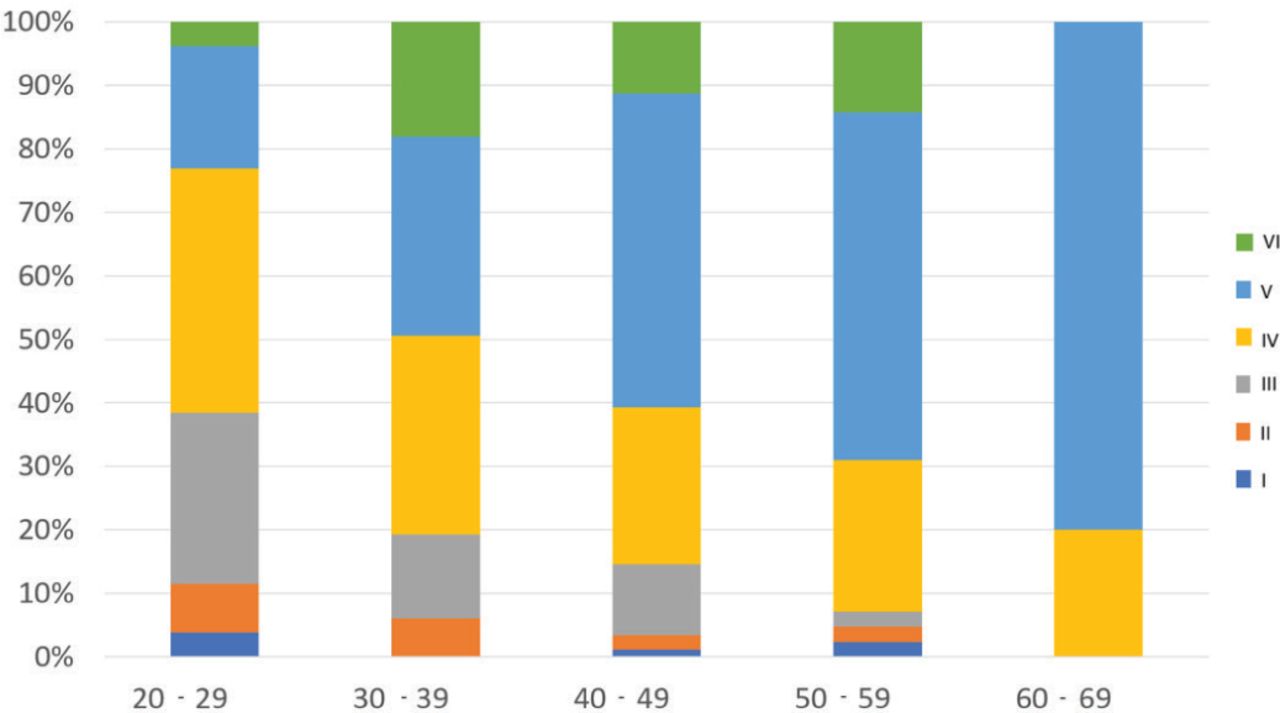
The prevalence of beard types also varied according to age group. It was observed that patients aged 20-29 have lower frequencies of types V and VI compared to other age groups. On the other hand, they show a higher concentration of types III and IV than the others. Types I and II are less frequent across all age groups. Type V, in particular, shows an increase in frequency as age increases. See Figure 9 for a better visual comparison.

Distribution of beard pattern by age group.
Another limiting factor of the studied population is that patients with an incipient beard and, in contrast, patients with a very full beard, tend to shave their existing beard more frequently, which made analysis difficult and led to the exclusion of some of these patients from the study. Likewise, it would be ideal for all patients to be evaluated with the same facial hair length, but this was not possible to achieve. Some patients also tend to adopt shaving styles that conceal the characteristics of beard presentation, creating hairless areas in the lateral infralabial region, and especially in the maxillary and zygomatic regions, which can hinder analysis (Figure 10).

A: The same patient at two different moments: shaved lateral infralabial and maxillary/zygomatic region (left) and without shaving region (right).
Many differences in hair presentation were also found in the cervical region; however, this description is beyond the scope of this study. Generally, we observed that the central region behaves differently from the lateral region, and the same applied to the suprahyoid and infrahyoid regions: when hair appears in the chin region, it starts to extend into the central cervical region before developing in the lateral regions. In other cases, hair areas appear simultaneously in the central and lateral regions, with a lack of hair between the two areas. Similarly, some patients exhibit high hair density in the suprahyoid cervical region but low density in the infrahyoid region. In some cases, the hair extends through the thyroid cartilage region, meeting the chest hair (Figure 11).

A: Beard in the central segment of the cervical region; B: hair areas appear simultaneously in the central and lateral regions, with a lack of hair between the two; C: central region with high density in the cervical suprahyoid region, but low density in the infrahyoid region; D: the beard hair extends through the thyroid cartilage region, into the chest hair.
The behavior of the hairs in the cervical region usually follows the progressive increase of facial hair; however, we did not find a precise correlation between the presentation of facial beard and the characteristics of cervical beard in all studied patients: some type III patients may have dense cervical beard, while some type V patients can have sparsely filled cervical beard (Figure 12).

Type III with dense and extensive cervical beard (left) and type V with poor density on the infrahyoid region (right).
CONCLUSION
We have presented a morphological and progressive classification of men’s facial beard that is easily applicable across different population groups. In our sample of 250 males, the most frequent pattern was type V (42.4%, n = 106). Additional studies with larger samples are needed to investigate the statistical difference between each type described in different populations. This classification may facilitate the comparison of beard hair density in different populations with various phenotypic types. Like any morphological classification, there may be some confusion regarding the classification of individuals with borderline characteristics in each group; however, in the studied population, the classification was efficiently applied.
- Copyright © 2024 by the International Society of Hair Restoration Surgery
This article is open access and may not be copied, distributed, or modified without written permission from the International Society of Hair Restoration Surgery.
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.