

Introduction
Most traditional hair transplant techniques require two to four sessions into the same, initially bald, recipient area to provide sufficient hair density over a large enough area to be cosmetically acceptable to the majority of patients. The need to return for these multiple sessions leads to multiple times off work, multiple cosmetic recovery times, more pre-operative anxiety, and more post-operative discomfort for the patient.
Wouldn't it be more convenient for the patient if an adequate density of transplanted hair could be achieved over a (traditionally-sized) targeted recipient area in just one session of hair transplantation?
Wouldn't it be more convenient for the patient if an adequate density of transplanted hair could be achieved over a (traditionally-sized) targeted recipient area in just one session of hair transplantation? Hence, the rationale for the “one-pass hair transplant.” This article will summarize its evolution, its benefits, and how the author has overcome myriad technical difficulties encountered during the development of this technique.
The Concept
The author will never forget hearing a question posed to a panel of experts at a hair transplant convention in Rio de Janeiro in 1992. The question was: “Which of the four (standard graft) sessions required to complete a hair transplant grows the best?” What was amazing was the confidence of the delivery of an emphatic and absolute answer that, without any thought or hesitation, came straight from the mouth of Dr. Martin Unger: “The first. The first session always grows the best.” This revelation was the inspiration to devise a method in which the “first session” into an area would be the only session required.
The Hypothesis of Less Scarring Leading to Better Growth
One can hypothesize that scarring, or “microscarring” in the case of follicular units, forms after each session of hair transplantation in at least a proportion of patients. This scarring impairs the vascularity of the area transplanted. This hypothesis implies that better growth may be obtained by planting, say, 100 grafts into a given “virgin” area once (provided the vascularity was not impaired), than by planting 50 grafts into the same sized area in an initial session, and then a second 50 grafts later during a second session into the same area. Clinical studies are currently underway, and preliminary findings so far tend to support this hypothesis. Proof of this hypothesis would be a very strong argument in favor of the one-pass technique.

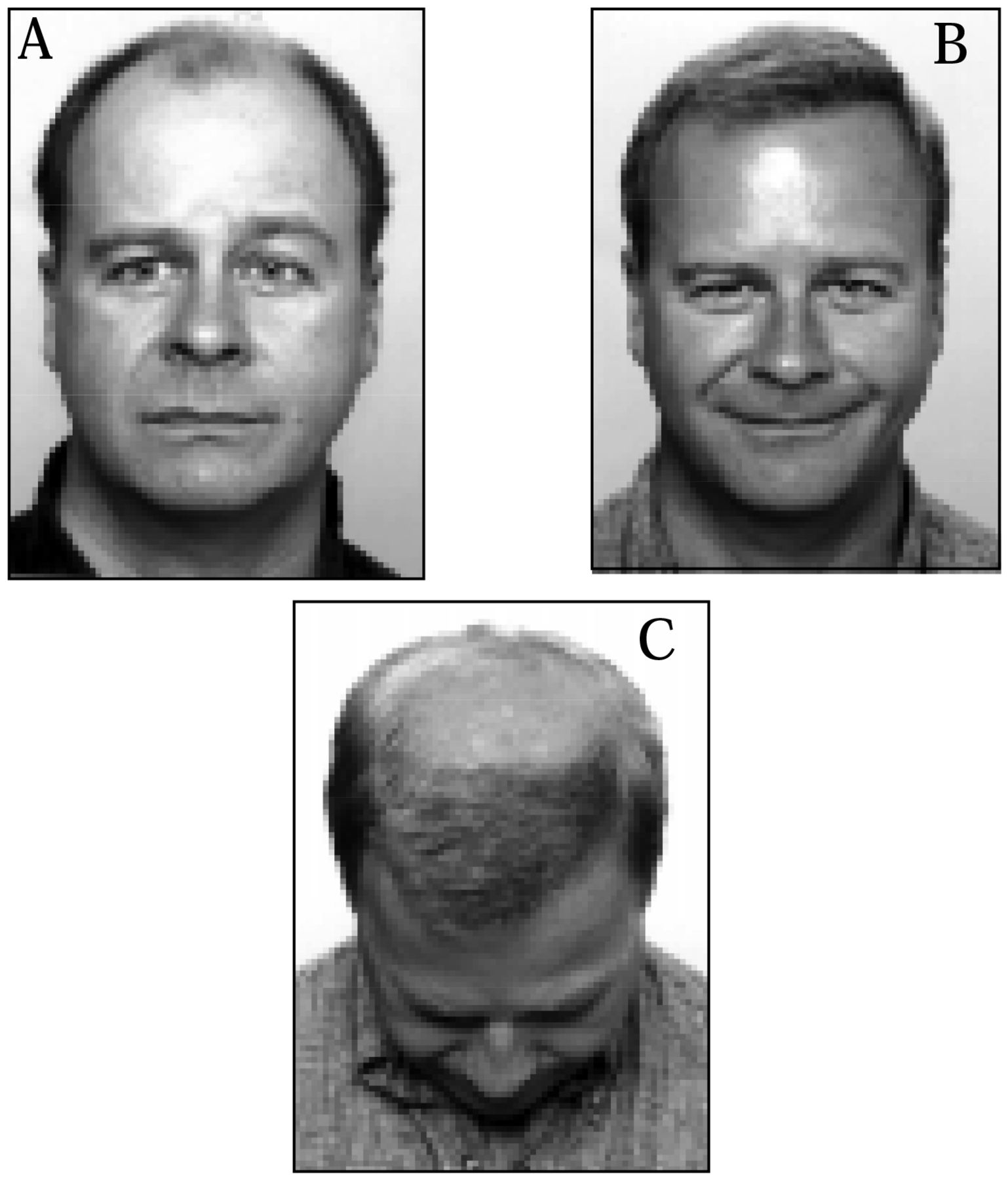
Photographs taken before (1A) and 12 months after one pass of 3,098 follicular unit grafts (1B, 1C). Figure 1C demonstrates typical coverage of the “front third” of the scalp.
Evolution of the One-Pass Technique Method
In October of 1995, the author and his staff learned how to perform FU transplantation from Dr. Bobby Limmer. Initially, 500 to 1,000 grafts were transplanted per session. Over the next 18 months, sessions grew in size both in terms of increasing numbers of grafts and increasing density of placement. By 1997, we were routinely performing “megasessions” of 3,000+ grafts placed to an average density of 37 follicular units/cm2 over an area of about 80cm2. For all except the patients with Norwood Stage VII with broad heads and narrow temporal fringes, 80cm2 covers the frontal third of the bald area of the scalp (Figures 1A–C). Thus, since 1997, the author and his staff have been able to cover the front third of the bald or thinning scalp with 3,000 grafts in one pass, achieving sufficient density to “frame the patient's face” to virtually all patients' satisfaction.
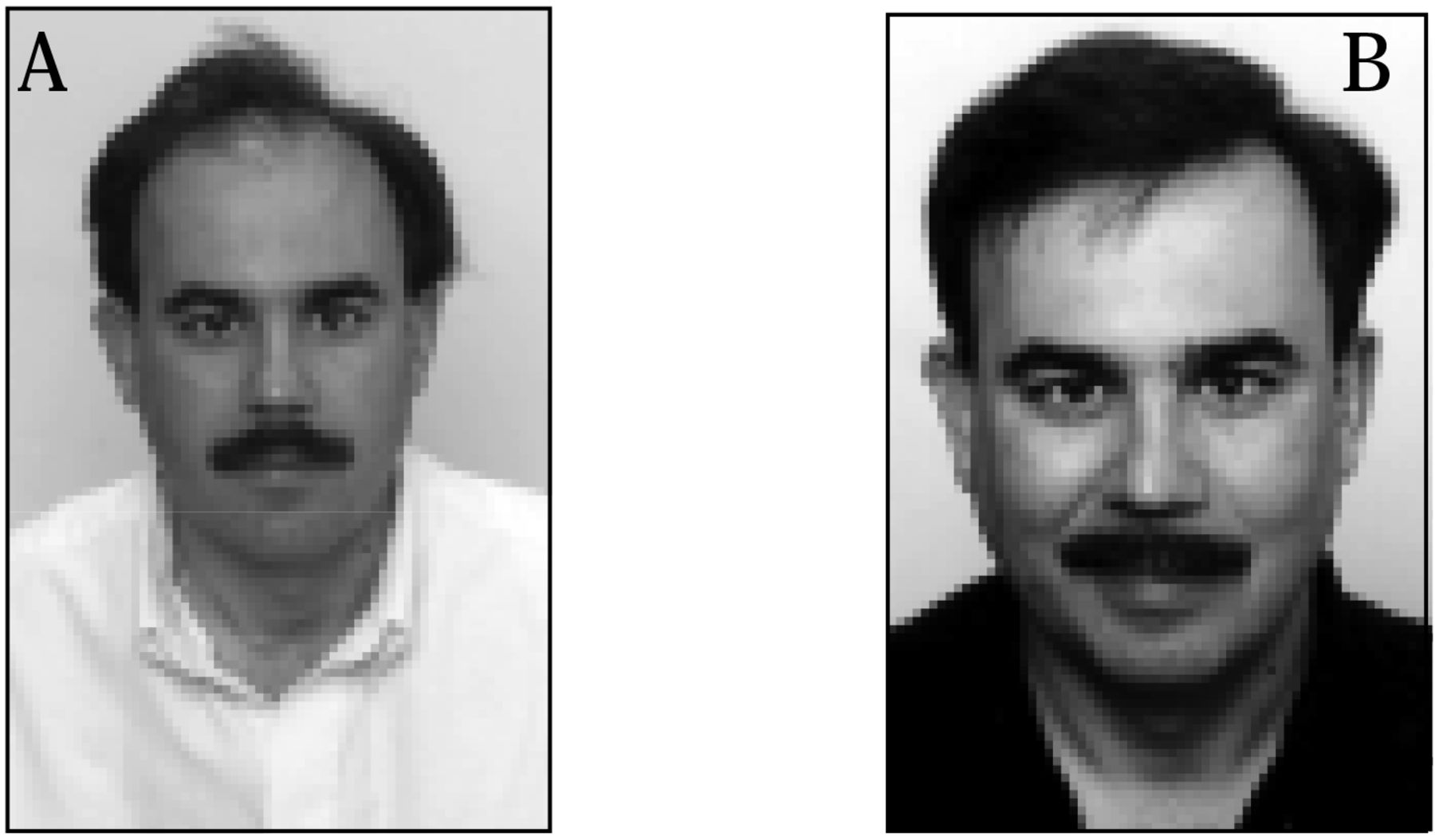
Patients with typical resulting densities are displayed in Figures 2 and 3. Density, of course, tends to be greater in patients with donor hair that is coarse and in those with a higher percentage of multiple-haired FUs.

Results of transplantation of coarse hair. Photographs taken before (2A) and 9 months after one pass of 2,050 follicular unit grafts in 1997 (2B).

Results of transplantation of hair with average shaft diameter. Photographs taken before (3A) and 2 years after one pass of 2,533 follicular unit grafts (3B).
Size of Currently Performed Megasessions
It is seldom that more than 3,000 grafts are transplanted in one session. The donor scalp of average density rarely yields more than an average of 100 follicular units per cm2, and removing more than 30cm2 of donor area can be problematic. One tries to keep the anterior ends of the donor incision posterior to the superficial temporal arteries, which in most patients limits the donor strip to 28cm in length. If one tries to keep the average donor strip width to less than 1.2cm, then one is usually limited to sessions of about 3,000 grafts or fewer. Wider donor strips, in most patients, risk wider scars. It generally takes 8 to 12 hours to transplant 3,000 grafts in one session. Sessions of more than 3,000 grafts can be very exacting and exhausting for both patient and staff, particularly if there is bleeding and popping.
Benefits of the One-Pass Technique
Increased Patient Convenience
The increase in convenience for the patient of the one-pass technique is enormous. Less down time from work, because of fewer sessions, translates into enormous financial savings for the busy wage earner. Also, having fewer sessions usually means lower total costs, so far as professional fees go. The optimal cosmetic benefit of the patient's hair replacement surgery is obtained earlier because it occurs 8 to 10 months after the first session, instead of 8 to 10 months after the last session. Additional advantages of fewer sessions are less total anxiety, less total post-operative discomfort, and less time when it could be evident to the patient's friends, family, and co-workers that the patient has been undergoing hair transplantation. In the case of the patient who chooses to have his or her hair transplant performed by a distantly located surgeon, there will be much less traveling involved.
Better Donor Area Management with Less Scarring
The traditional hair transplant method for excising donor strips has three main problems that the one-pass technique addresses. In the traditional hair transplant method, a second strip taken from the donor area can stretch wider a donor scar superior or inferior to it. For example, when removing a second strip above or below the scar from the first strip, the original scar from the first strip usually gets stretched wider by the pulling together of the wound edges during closure of the second strip. A scar that started off looking extremely narrow, will, after several sessions where donor strips have been taken above or below, look much more conspicuous. In addition, the scar from the first strip can tether the skin so that there is more tension when closing the edges of the second strip.
There is also less hair available to cover existing scars each time a new donor strip is excised. When several short scars are created one above the other in a ladder-like fashion, there will be less hair coming down from above to cover the lower scars.
Finally, each time one excises a new donor strip, the ends traditionally must be tapered. It is more difficult to avoid transecting hairs while excising a tapered end. These unavoidably transected hairs will likely not regrow, leaving bare or thin areas of skin that look like scars.
In the one-pass technique, all three of these issues are addressed. One long donor strip is excised from ear to ear. There will be only one scar and fewer tapered ends overall, the latter resulting in fewer transected hairs.
Reduced Potential for Inaccurate (or Dishonest) Estimation at Consultation of the Total Number of Grafts and Total Ultimate Cost to the Patient
Inherent in the traditional multiple-session method is the potential for deceptive marketing when the patient inquires, “How many sessions will I need?” A dishonest physician or salesperson could answer in a variety of encouraging but misleading ways, such as “…two sessions are usually enough to please 90% of my patients, but about 10% may want an additional third session…,” when the surgeon or salesperson knows perfectly well that at least three or even four sessions will probably be necessary to please most patients.
With the one-pass technique, at the initial consultation the physician draws the perimeter of the area to be grafted (with, say, 3,000 grafts) and points to either a live model present and/or photographs to illustrate the density to be achieved with the one densely packed session of hair transplantation being offered. If the patient does not ultimately actually grow hair of that demonstrated density, then a second hair transplant session in the same recipient area to increase the density is offered at no extra charge. This extra session has been required in less than 1% of cases so far. Before predicting density, the physician must carefully assess the donor hair characteristics, including hair shaft diameter and the ratio of 3- to 1-haired follicular units in the donor area. It is better to first provide a conservative prediction then it is to over-promise.
Difficulties Performing the One-Pass Technique
Most hair transplant physicians attempting a one-pass hair transplant have difficulty placing the grafts closely enough together to provide adequate density (without compromising the vascularity of the area). When this difficulty is overcome, there are myriad difficulties in coping with the enormous number of grafts required to cover a large enough area to provide a worthwhile cosmetic benefit. These significant difficulties are probably the reason why the one-pass technique hair transplant has not been adopted and promoted by more hair transplant practitioners.
Dense Packing
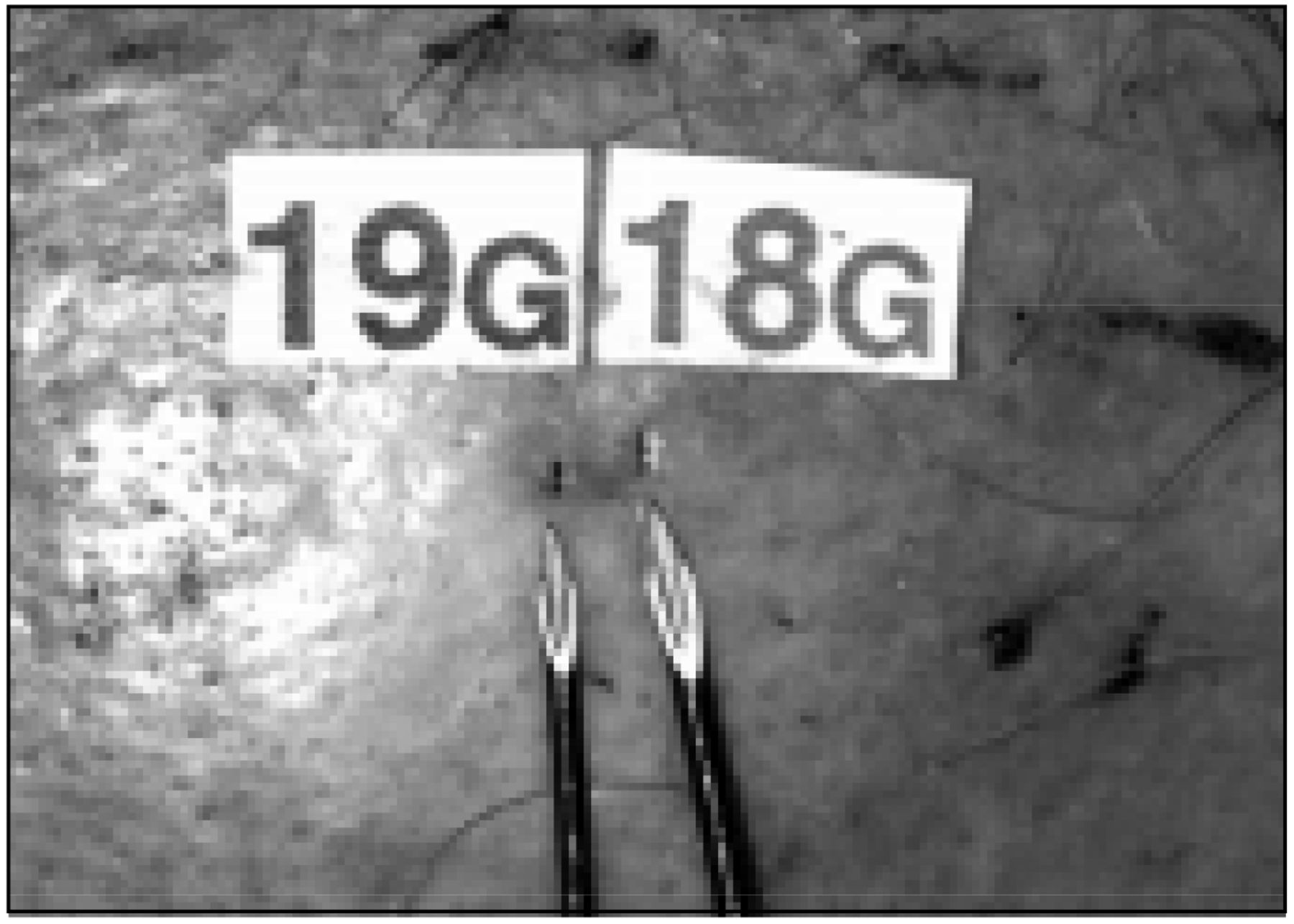
Some studies have demonstrated that dense packing over 40 follicular units per cm2 results in poorer growth. Most of these studies, however, have used 18-gauge needles (Stough, Orlando, 2000; Bill Reed, presentation in Puerto Vallarta, 2001). The secret of success in dense packing is to use as small a recipient site as possible. This necessitates using a 19-gauge hypodermic needle or smaller. An 18-gauge hypodermic needle simply produces too much vascular damage per incision for the necessary number of incisions per cm2. In other words, 40 incisions the size of an 18-gauge needle site will cause MUCH more vascular embarrassment than would 40 incisions the size of a 19-gauge needle in the same 1cm2 area (Figure 4). This increased vascular damage, with 18-gauge needles, is what in practice makes the difference between success and failure of attempts at dense packing, and what invalidates most of the previous trials demonstrating poor survival after dense packing.

Photographs demonstrating the difference in diameters of 19-gauge and 18-gauge needles and the resulting difference in the size of recipient tunnels.
The author favors the “stick-and-place” method of planting. With this method, the needle used to make the recipient site is first used as a dilator; and then, as the needle is being withdrawn, it is used as a shoehorn to help guide the graft into the minute recipient tunnel. The author believes that, in the majority of patients, it is technically impossible to plant large numbers of 2–3-haired follicular unit grafts of hair with average shaft diameter greater than 70 microns into 19-gauge hypodermic needle sites, as closely as it is routinely done in the author's practice, without the use of stick-and-place planting (Figure 5).
Knowledge of the above two crucial factors alone will not enable a hair transplant facility to successfully dense pack grafts. Implementation of theory into practice is extremely difficult. Exceptional natural talent and around 18 months of constant tutored practice are required before the long learning curve gets mastered, and staff members become expert at these techniques.

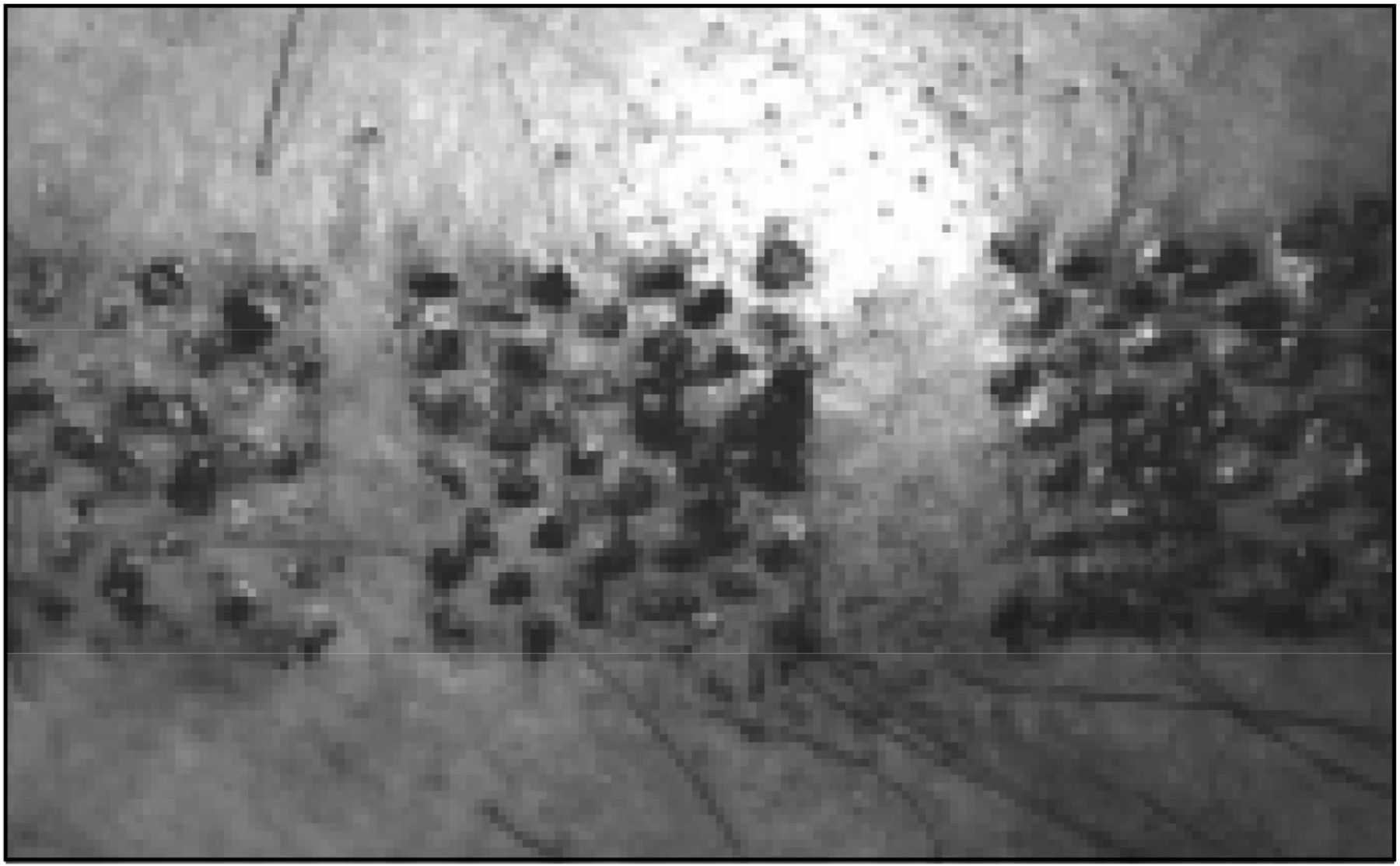
Photograph showing different densities of graft placement using the stick-and-place method. From the top square to the bottom square there are 45, 40, and 35 grafts per square centimeter.
Staff Recruitment and Training
Many technicians whose manual dexterity skills are good enough to plant minigrafts may never be able to successfully densely pack follicular units. Recruiting staff with the right qualities is difficult and time consuming. Long probationary periods are mandatory. A technician may seem talented at first, and may show steady initial improvement in the beginning months. All too often, however, after a 3- or 4-month period, his or her progress plateaus, and it gradually becomes obvious that he or she will never be able to dense pack follicular unit micrografts expertly.
Technical expertise is not the only quality required. The mental and physical fortitude to concentrate intensely on a repetitive, tedious task, and to be able to emotionally tolerate rigorous, critical ongoing quality control are other rare qualities a good technician must possess. Additionally, the successful technician must have a personality suitable to working harmoniously and without friction closely for long hours with his or her teammates. Staff selection and training is the most difficult and expensive component of the whole enterprise.
Prolonged Duration of Densely-Packed Megasessions
One must also be prepared to accept that, even with highly trained and efficient staff, it usually takes twice as long to dense pack the same number of grafts to a density of 35 to 40 follicular units/cm2 as it does to place the grafts more loosely planted (say 20 to 25 follicular units/cm2) into pre-made recipient sites. Because of this inherently slower planting technique, and with the greater number of grafts required, the surgery time of these sessions can be extremely prolonged.
Difficulties Specifically Associated with Follicular Unit Transplants
These include the need for binocular stereoscopic microscope dissection, skillful atraumatic graft planting, and, above all, the need to keep the grafts completely moist. The latter is by far the most important factor influencing the success of FU transplantation. Partial drying of grafts is the most common reason why so many practitioners are unable to get good growth from FU transplantation, despite otherwise excellent technique. The author feels strongly that these grafts must remain totally immersed in saline, rather than simply sitting atop a moist pad, if high hair growth rates are to be realized.
Difficulties Specific to Large Prolonged Megasessions
Practical Problems Related to Staff
In addition to the extra recruitment and training, there is the problem of staffing the clinic for the prolonged hours that the longer sessions take. Aside from overcoming the staff's dislike of working long hours day after day, planting for many hours on a daily basis can and does lead to physical ailments, such as “repetitive strain syndrome.” To combat this, close attention must be paid to ergonomics. For instance, it is important that planters rest either their elbows or forearms on a firm supporting surface while planting with wrist and finger movements. If the planters have to support the entire weight of their arms throughout their planting, they will often develop muscle strains in their neck, shoulders, and forearms. Older and slightly built staff who have been working at this for years seem to be especially prone. The planting staff must also rotate duties; that is, after a certain interval of planting, they should do some other type of work, such as cutting grafts or administrative work, prior to returning to their graft planting. They must have frequent relaxation breaks; and they must do regular stretching exercises at least every hour during their planting and cutting of grafts.
Bleeding and Popping
Bleeding and popping, which are tolerable nuisances in small or intermediate-sized sessions, can cause almost insurmountable difficulty in a large megasession.
Advising patients not to do any vigorous workouts for one week before surgery can greatly help reduce bleeding. We also give each patient an injection of Vitamin K as early as possible on the morning of surgery, or better still, the day before surgery, if possible. We try to avoid infiltrating Lidocaine directly into the operative field. It is a vasodilator, and therefore increases bleeding because the half-life of Lidocaine is longer than the half-life of Adrenaline. We therefore use supra-orbital and supra-trochlear nerve blocks and a ring block and/or field block. We infiltrate the recipient area with either 1:100,000 or 1:50,000 Adrenaline saline solution. If we use 1:50,000 Adrenaline solution, we do not infiltrate the entire recipient area at once, instead we infiltrate a small area the size of a quarter or a silver dollar prior to that area being planted, while a similar area that had already been infiltrated is planted.
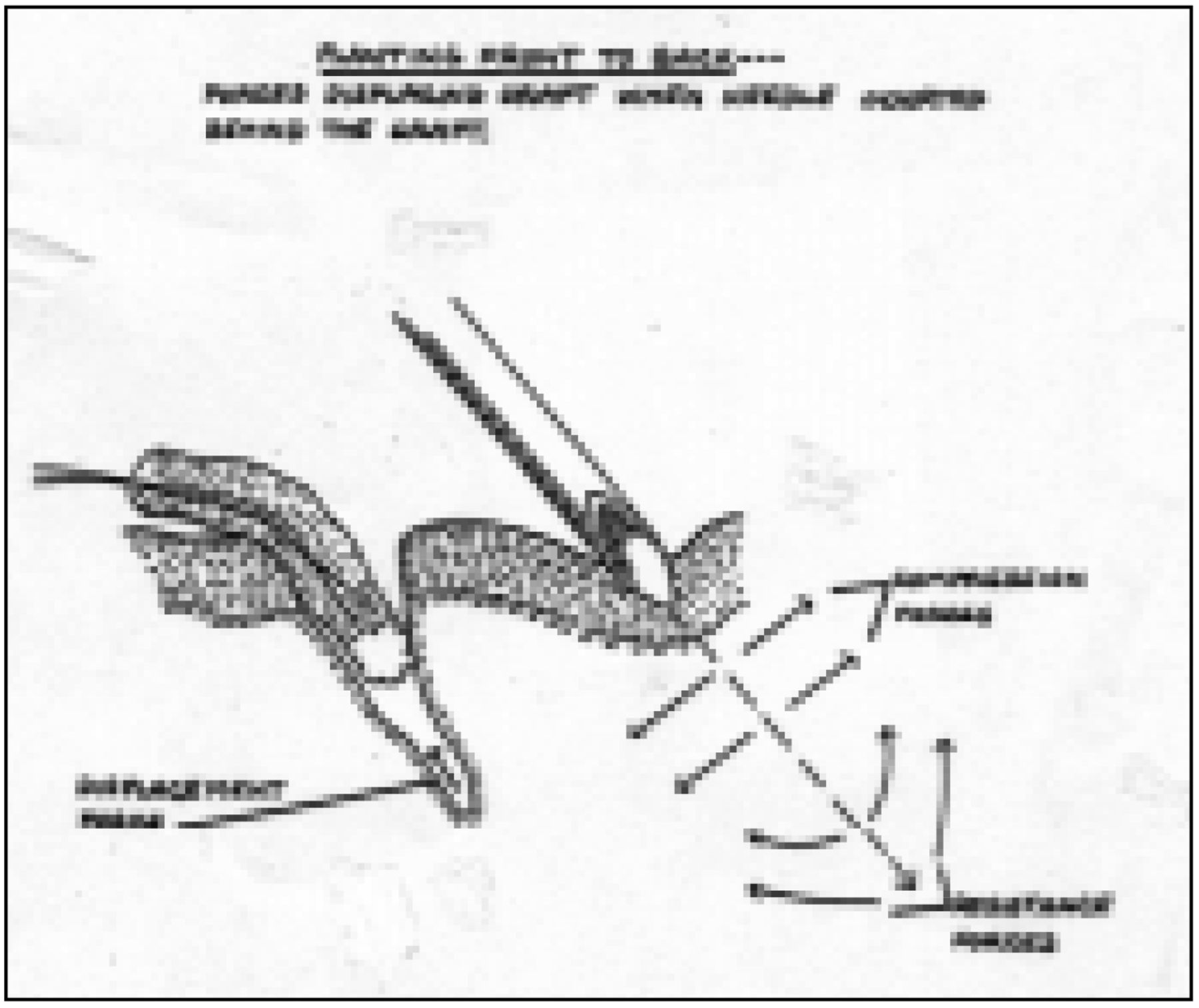
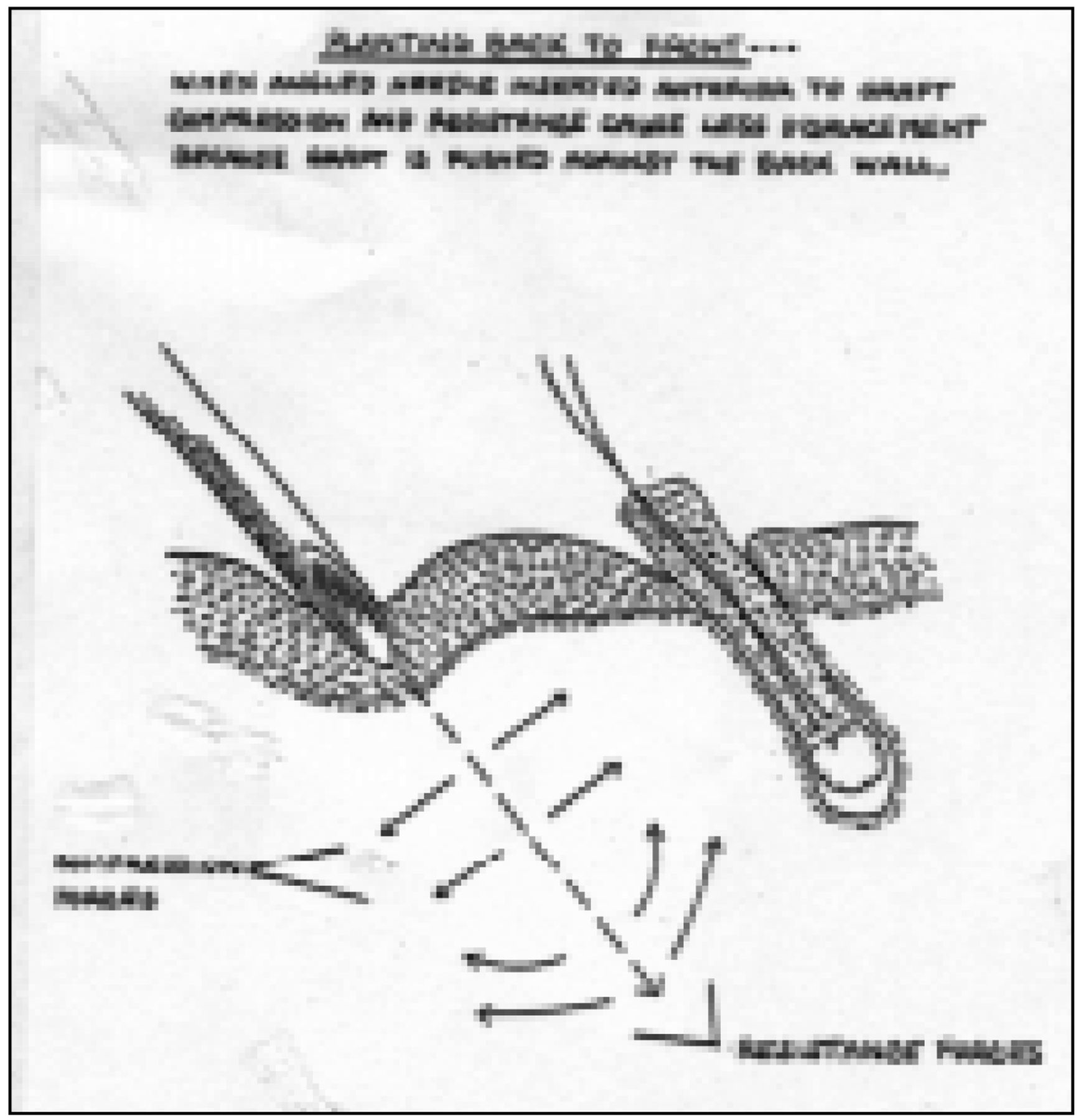
Popping can also be very frustrating and can prolong surgery. Popping, of course, refers to previously transplanted grafts “popping” out of the skin during the transplantation of a new graft. If the patient's skin characteristics lead to popping, we try varying the recipient site size or trimming the grafts a little narrower or not trimming them as much. Another approach to popping is to reduce the density of the planting; i.e., to space the grafts further apart. A third method of reducing popping is to plant from the back of the recipient area to the front. This makes it easier to hold the previously planted grafts in place with gentle pressure while the next recipient site is created (Figure 6). If one attempts to hold down previously planted grafts while planting from front to back, the fingers obstruct proper needle placement. Planting from back to front also prevents the skin resistance forces from acting in a direction that would displace the previously placed grafts (Figures 7 and 8).

Photograph demonstrating how planting from back to front allows previously planted grafts to be gently held in place with gauze.

When planting from front to back, skin forces tend to displace the graft when the needle is inserted behind it.
Dehydration and Hypoglycemia
Without attention to nutrition and hydration, many patients feel weak and faint toward the end of the day. Dehydration and hypoglycemia can be avoided by encouraging the patient to drink large amounts of either fruit juice or pop, and by making sure that they have ample meals, including breakfast, mid-morning snack, lunch, and when applicable, an early supper.

When planting from back to front, there are less displacement forces on the graft when the angled needle is inserted in front of the graft. Some forces push the graft against the back wall.
Prevention of Deep Vein Thrombosis
If patients have spent a long time traveling to have surgery, that is, more than a 5-hour drive or flight within a day of their hair transplant, one should bear in mind the potential for deep vein thrombosis. This is especially so if there is a prior history of deep vein thrombosis, or if the patient has other risk factors. One should ambulate the patient, walk them around the office at meal times, and possibly additionally in between meals. At-risk patients should also wear elastic support stockings and should exercise their legs between walks. Such patients should be advised not to fly in and out on the same day as the surgery.
Lidocaine Toxicity
Larger and more prolonged sessions require larger total doses of Lidocaine. One has to ensure that the total dose of Lidocaine doesn't mount up to what could become toxic. However, it probably doesn't matter very much if slightly greater than the “maximum allowable amount of Lidocaine” is given throughout a 12-hour megasession period. The usually quoted maximum amounts allowable were assessed on the basis of surgeries of shorter duration. With the short half-life of Lidocaine, most of the Lidocaine that was given earlier on in the 12-hour surgery would be metabolized before Lidocaine administered toward the end of these lengthy surgeries.
Throughout the planting of the hair transplant, the patient usually lies back at approximately 45 degrees in a dental chair, putting pressure on the donor area. When the local anesthesia in the donor area wears off, these patients usually complain that the back of their head is painful as they lie on it. Re-anaesthetizing them with Lidoocaine is an easy quick-fix, but tachyphylaxis occurs, and they need more and more frequent infiltration into the donor area. This can cause cumulatively enormous amounts of Lidocaine to be used. It is better to try to put a wedge under the patients' neck to keep their head propped up so that the donor area does not bear the weight and pressure of their head against the backrest of the chair/operating table. If this is not possible, then depending upon the amount of Lidocaine used so far, and the projected amount that may need to be used throughout the rest of the session, it may be better to give a narcotic analgesia rather than keep on using more and more Lidocaine in this area.
Orthostatic Hypotension, Nausea, and Vomiting
Lastly, toward the end of large megasessions, some patients tend to develop post-operative orthostatic hypotension, getting nauseous and vomiting when they sit up or stand. The etiology of this is unknown, but it seems to be related to volume depletion, excessive administration of Benzodiazepines and/or narcotics, and increased vagal tone. It frequently occurs, however, in the absence of one or more of these purported factors. Prevention of nausea and vomiting with postural hypotension can be achieved by preventing the patients from becoming volume depleted and ensuring adequate fluid intake. If the patient is reluctant to drink or is too sedated to readily drink, then intravenous fluids such as normal saline should be administered. It is important to minimize medications/drugs as much as possible. The more Benzodiazepines and narcotics a patient has, the more likely they are to get orthostatic hypotension and nausea at the end of a prolonged hair transplant. Patients should also be mobilized actively toward the end of their surgery. In other words, rather than allow them to remain immobile and almost horizontal for 8, 10, or 12 hours, and then at the end of the procedure suddenly have them stand erect, it is better to make sure they get up and walk around at various time intervals, such as when they have their snacks, juices, and so on.
Also, during the last hour or so of their surgery, the patient should sit forward with both feet on the floor while the planters, who will need to stand, finish their work.
Conclusion
So, is the one-pass technique preferable to traditional multiple sessions? From the patient's perspective, it definitely is. From most doctors' perspectives, it probably is not, as it is fraught with technical difficulties and has a much steeper and longer learning curve. The large and prolonged sessions produce staffing and management problems, as well as being extremely personally onerous for the physician. Finally, the longer staff training and recruitment time and the extra staff hours required for the slower and more labor-intensive method make the one-pass technique less financially profitable.
In the past five years, the patients' and the author's satisfaction with the results of the one-pass technique hair transplant have more than made up for the challenges of this difficult, new technique, which is vastly more convenient for the patient. The results of the one session consistently look spectacular, and the patients are delighted!
- Copyright © 2002 by the International Society of Hair Restoration Surgery
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.