

Introduction
For patients with less than desirable aesthetic hairlines from prior hair transplantation, the most common recommended method for repair is further grafting. The concept is that the additional grafts that are theoretically performed in a more refined approach will conceal the old grafts. This approach can be quite useful, especially when the transplanted hairline as it presents is sufficiently high enough to allow for at least 10-15mm of further advancing with new grafting, and there is sufficient donor hair grafts. I have utilized this grafting technique in the great majority of the more than 1,500 revision procedures I have performed over the past 15-plus years, with very good to rather impressive outcomes in the large majority. In approximately half of these grafting cases, a small number of the most unaesthetic grafts (anywhere from 20 to as many as 50 or so) also need to be removed to achieve a more natural appearance, especially for those along the frontal-most hairline that are very noticeable due to size (3 or more hairs), angulation (too perpendicular), pitting of the surrounding skin, or poor location (placed too far forward and/or surrounded by scarring such as pitting or hypopigmentation).
There are certain circumstances, however, when further grafting is not the simple solution to the problem. As effective as this technique can be in many patients, in others it simply is not going to improve hairline aesthetics sufficiently to allow the patient to regain the natural look he greatly wants. This is particularly true in those patients with several aesthetic problems that include:
hairlines that are too low or too flat (rounded instead of receded frontotemporal recessions);
a large number of unnatural appearing grafts that cannot be concealed with further grafting; whether because of poor angulation, large size, or other aesthetic issues; and
scarring of the surrounding skin from the prior placed grafts or from well-intentioned but unsuccessful efforts to improve appearances by graft removal and/or further grafting.
It is in these patients that one of the following three alternative procedures can and should be offered:
Linear excision of the entire or portion of the hairline.
FUE punch removal of prior placed hairline grafts.
Fusiform-shaped scalp reduction performed just behind the hairline.
One particular motivation for writing this article is to demonstrate the proper method and applications of these techniques. I do not take credit for inventing these techniques, for I have learned the basics of them from some of my more respected colleagues (such as Drs. Dow Stough and Shelly Kabaker), but I have modified them to allow them to achieve the most impressive results. Performed properly, these techniques have made a huge difference in the lives of some of my patients, allowing them to no longer need to continually worry about their unnatural appearance.
Linear Excision of the Hairline—Partial and Complete
Almost 11 years ago, I was faced with a very challenging case of a male who 20 years earlier underwent a series of plug and minigraft transplanting to create a 2.5cm-wide hairline that unfortunately was too flat and too far forward—just 7cm above the nasion. Another surgeon had attempted to remove some of the larger of the 700 or so grafts that contained 3-7 hairs each, which resulted in unaesthetic hypopigmented scarring in place of the grafts. The patient was resigned to wearing a hairpiece, unless something heroic was performed for him.
It was in this rather desperate situation, with essentially nothing left to lose (he was going to have to wear a hairpiece otherwise), that led me to recommend what at that time I considered a rather invasive procedure—complete excision of the entire 2.5cm-wide hairline, then reapproximating the defect with suture closure—essentially performing a browlift without the forehead undermining that would be performed to elevate the brows. The prior transplanted hairs contained in this removed strip were dissected out then replanted higher up into the frontal forelock. The scar healed up beautifully, and the patient chose not to have the offered second procedure of grafting into the residual hairline scar once it matured, something I now perform in the majority of these patients.
What made this patient an appropriate candidate, and others like him, were several features. First, the patient really had no other options, other than to wear a hairpiece. As I have performed more and more of them and have developed more confidence in the results, I no longer have this as a requirement. Second, the patient had a decent amount of laxity of the forehead/hairline region, allowing for the removal of the entire transplanted hairline without significant tension on the closure. Third, and very important, the skin along the hairline was also damaged due to scarring from a combination of the prior large grafts and previous attempts to remove the grafts using larger punches. Other important indicators for success include prior attempts at plug removal that simply didn’t do enough, and in certain patients, brow ptosis that can be addressed simultaneously with the hairline excision.
While this patient had his entire hairline excised, in approximately one-third of patients, only a portion of the hairline is excised. Most commonly, this will be in the frontotemporal recessions, where the typical patient had poorly placed grafts making the hairline appear too flat. With these partial hairline excisions, the width of fronto-temporal scalp excised can be as much as 3.5cm, depending upon the laxity of the scalp, the width of the scalp in this area that is scarred and/or containing of unaesthetic grafts, and whether performed bilaterally (where there will be more tension due to the additional vector of pull) or unilaterally. These partial hairline excisions are performed bilaterally most common, sparing as much as 8cm of the frontal-most hairline.
Whether unilateral or bilateral, the technique is similar. An incision is made right along the leading edge of the affected hairline, then the forehead skin is undermined 3cm or so forward in the subfrontalis muscle plane, then pulled back up to assess how much of the hairline can then be excised. If a browlift is being performed as well, this undermining of forehead skin is extended to the region of the brows to free them up for elevation. The excess hairline skin—hair grafts and all—is removed, and the defect is sutured closed with 2-0 Vicryl to the frontalis/galeal layers, then sometimes with 4-0 chromic to the superficial subcutaneous layer, then with a running 6-0 nylon to reapproximate the skin. To achieve a less detectable nonlinear scar, both incisions are made in a rolling irregular fashion, almost like a “soft” w-plasty.
Bruising and swelling are usually quite minimal unless the browlift is performed. These procedures, even when incorporating a browlift, are usually performed under local anesthesia with, if desired, oral sedation. If the proce-dure is being performed without a browlift, limited undermining of the forehead skin to no further than 3cm results in little to no brow elevation, which is something that surprised me at first. The prior transplanted grafts that are contained in the excised hairline skin can be dissected out and re-transplanted into another part of the scalp at the same procedure.
Case Examples
1. 55-year-old man, presented 18 years’ status post approximately 200 plug grafts, transplanted into two rows. After full presentation of risks and benefits, patient opted to undergo a linear excision of the entire hairline that contained the grafts, with simultaneous transplanting of almost 700 grafts to the frontal forelock region. Two years later he underwent a second hair grafting procedure of 1,100 grafts, where grafts were concentrated along the fine-line incision scar as well as blending it into the frontal forelock. Photos taken 6 years after this second procedure.

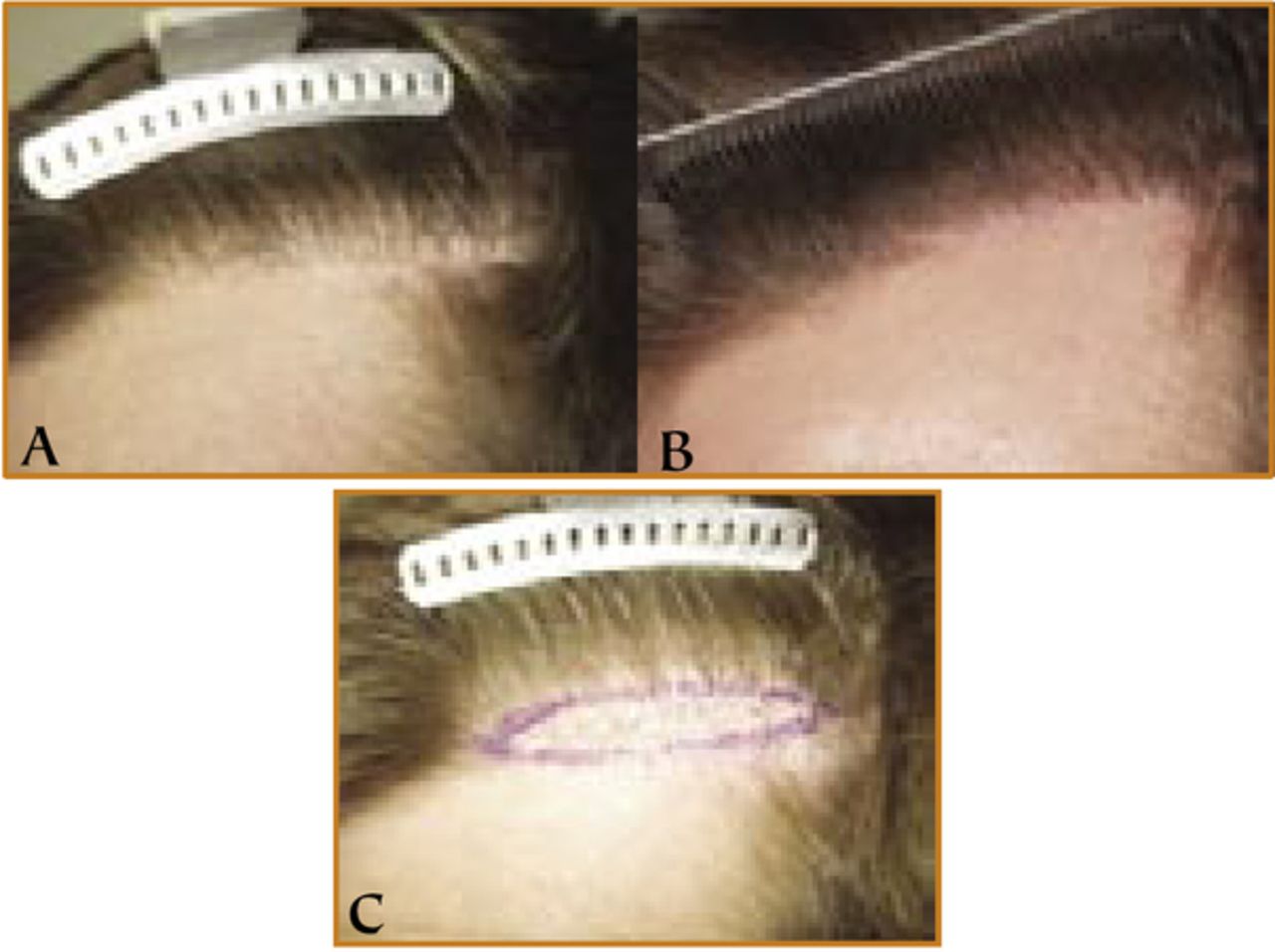
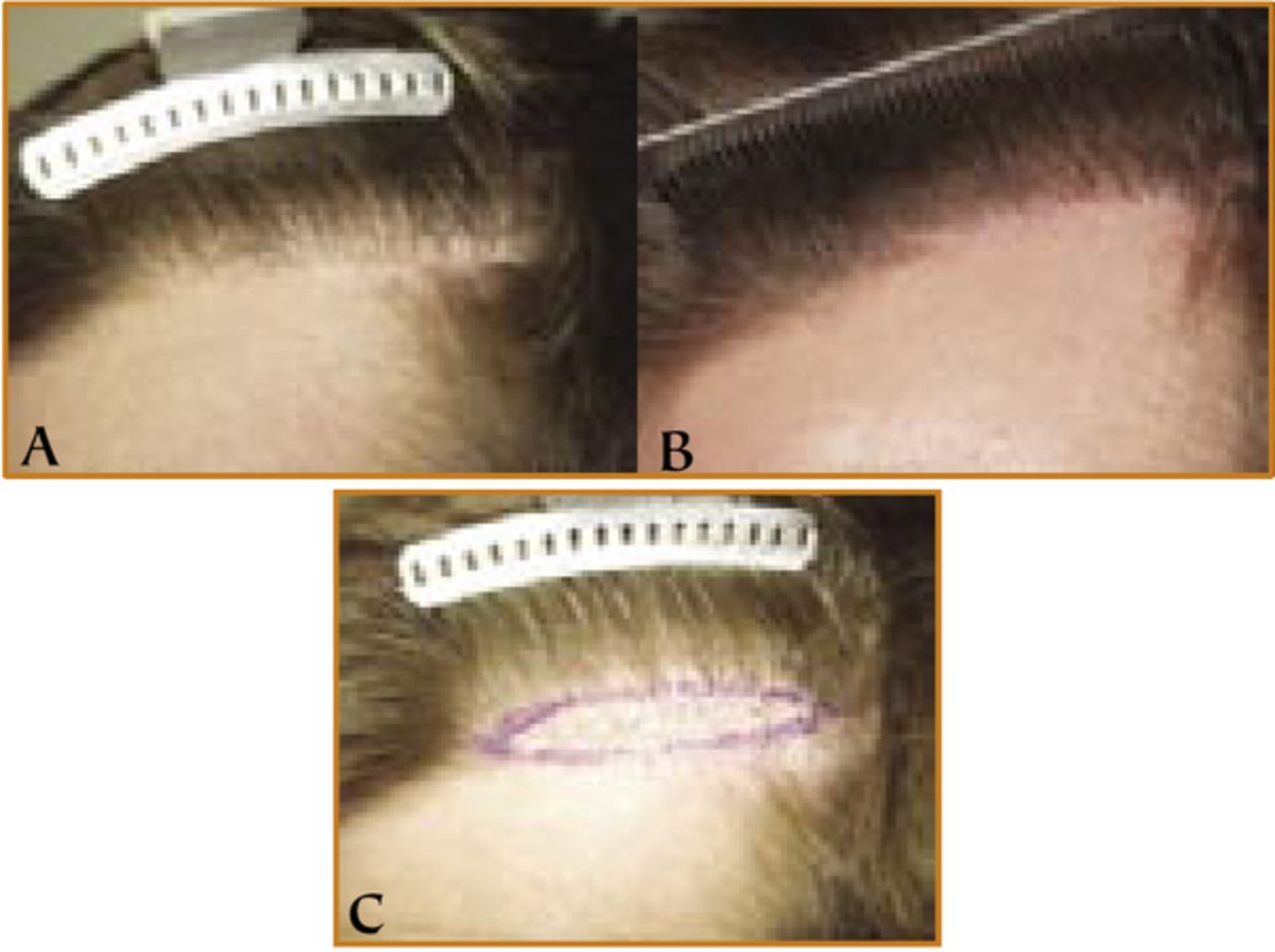
2. 22-year-old young man, presented 4 years’ status post approximately 400 micro-/minigrafts to bilateral frontotemporal recessions that he soon after regretted. One year earlier, he underwent (by another surgeon) two punch extraction procedures of the prior placed grafts that left his skin with more scarring and still a large percentage of transplanted hairs. Frustrated with the less than acceptable result, he underwent excision of the bilateral frontotemporal recessions (as marked) allowing the scarred skin and the remaining grafts to be excised.
Extensive FUE Punch Removal of Grafts
The fundamentals of this technique have been described in the past, but as primarily applied to larger grafts (4 or more hairs), and with certain limitations. Using follicular unit extraction instrumentation, a large number of grafts closely placed together can be removed, with little if any residual detectable scarring. FUE punches of 0.8mm and 1.0mm can be used to extract smaller grafts containing 1-2 hairs and larger grafts containing 2-4 hairs, respectively. The small size of the residual punch hole permits the extraction of hundreds of prior placed grafts in a single procedure; this technique can be used simultaneously with hair grafting in the area.
The biggest challenge to FUE punch extraction is that scarring and fibrosis of the transplanted grafts can some-times make removal difficult. In some cases not all the hairs in a graft get extracted, so patients are advised that they may desire a second procedure as soon as 2 months later to remove additional grafts. Healing of these extracted sites is quite rapid, with healing by secondary intention (no suturing required) of these 0.8 and 1.0mm punch sites taking place typically in less than a week, and any residual pinkness resolving over several more weeks.
Case Example
3. 44-year-old man, presented 1 year status post approximately 500 grafts to the hairline. His dark, thick donor hairs made the unnaturalness of these 1- to 5-hair grafts more obvious, with their perpendicular angulation and regular distribution appearing totally unnatural. He underwent a single FUE extraction procedure in which over 90% of these grafts were extracted, with the grafts dissected down into smaller follicular units and re-transplanted higher up into the frontal forelock.

Fusiform-Shaped Scalp Reduction Behind the Hairline
Instead of excising the grafts right along the hairline, in some circumstances a similar result can be achieved by performing, in essence, a scalp reduction(s) several centimeters behind the hairline. The main advantage of this technique is that it avoids making any incision along the hairline, which instead is pulled up/back from the fusiform scalp reduction incision. So while this technique improves the position of the hairline, it does not remove unaesthetic grafts or scarred skin along the hairline.
The most common indication for this procedure is for elevating the frontotemporal recessions, either unilaterally or bilaterally. If unilateral, just one scalp reduction incision, typically 4-6cm in length, is made behind the affected frontotemporal hairline, and if bilateral, two incisions are made, each one behind the frontotemporal hairlines. By placing the incisions close to the hairline, greater control of the amount of elevation is achieved, and if desired, asymmetric hairlines can be made more symmetric. In other cases, a single midline sagittal scalp reduction made several centimeters behind the frontal-most hairline can achieve a similar result of bilateral frontotemporal hairline elevation. In all of these cases, any prior transplanted hairs contained in the scalp reduction can be harvested and replanted.
Case Example
4. 49-year-old man presented status post a large number of hair grafts to the frontal region with a complaint primarily of his hairline being too flat. Bilateral scalp reductions each measuring approximately 2.5cm in width were performed to elevate the frontotemporal recessions by approximately 1.5cm. The hairs contained in the excised ellipses were dissected out, providing 180 grafts that were then planted along the hairline so as to soften the appearance.

Summary
The literature is replete with the descriptions of reparative techniques that involve further grafting sometimes combined with graft removal.1-4 For good reason (relative noninvasiveness and patient acceptance), these techniques are quite effective in the majority of patients. In a article that appeared in Facial Plastic Surgery Clinics, Vogel nicely described some of the techniques I have written about, in particular the entire hairline excision procedure.5 While a much more invasive technique, the appropriate patients simply see few options to having the procedure performed, whether due to scarring of the recipient area that needs to be completely excised or a hairline that is simply too low, and willingly undergoes the surgery that will potentially allow them to resume a life not restricted to the wearing of a hairpiece.
A note from Jim Vogel, MD Owings Mills, Maryland jevps{at}comcast.net
Dr. Epstein has summarized well his techniques and approach to repairing unsightly hair transplants due to poor surgical practice or outdated techniques, which are often made worse in the face of progressive hair loss. Corrective hair restoration surgery is a small but important subspecialty within our field. As Dr. Epstein has nicely demonstrated, these methods provide patients a tremendous improvement in self-esteem and a new lease on life.
The techniques presented are, admittedly, not new. However, what is relatively new in the armamentarium is the use of FUE in repair surgery. Dr. Epstein’s third case nicely illustrates the use of FUE in repair of un-sightly grafts. However, while FUE using 0.8mm or 1.0mm punches has the advantages mentioned in the article, larger plugs, which are 3-4mm, often require larger punches in the range of 2-3.5mm (I add an example to illustrate this comment). Surgeons should not be concerned with secondary healing of these larger excisions and be assured that a smaller punch will not be as effective in these circumstances.
A stated purpose of the article is to “demonstrate the proper applications of these techniques….” The fact is that many pluggy hairlines or hairline position problems require repair with surgical procedures that require significant surgical training and experience. Paradoxically, more invasive procedures often result in softer, more natural results than the less aggressive grafting procedures that created the unnatural appearance.

An example of a patient in whom a pluggy hairline was treated with linear excision and recycled grafts immediately planted into forelock and hairline. No separate donor harvest was performed. Eight months later additional intense 4mm plugs were removed with 3.5mm punches, and additional hairline grafting was performed using recycled hair and primary donor harvest. Final result is seen 18 months following the first procedure.
- Copyright © 2010 by The International Society of Hair Restoration Surgery
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.