

Introduction
As hair transplant surgeons, we often perseverate on aesthetic placement of grafts. However, getting grafts to grow optimally through effective wound healing is key to getting these good results whether one is discussing the donor area or the recipient zones.
Historically speaking, hair transplantation surgery was treated much like any other post-operative wound. The days of the whole head dressings, weeks of antibiotics, and punch grafts healing via secondary intention will bring a shudder of recognition to the experienced surgeon. More recently, the focus on minimally invasive techniques, scar minimization (through trichophytic closure and FUE most notably), and maintaining a moist (not wet OR dry) environment has improved both the wounds themselves and the patient experience. Without delving into extreme cases of poor wound healing, infection, or rare complications, following is an overview of the process and a point-by-point guide to optimizing wound care for your hair transplant patients.
Physiology of Wound Healing: A Quick Review
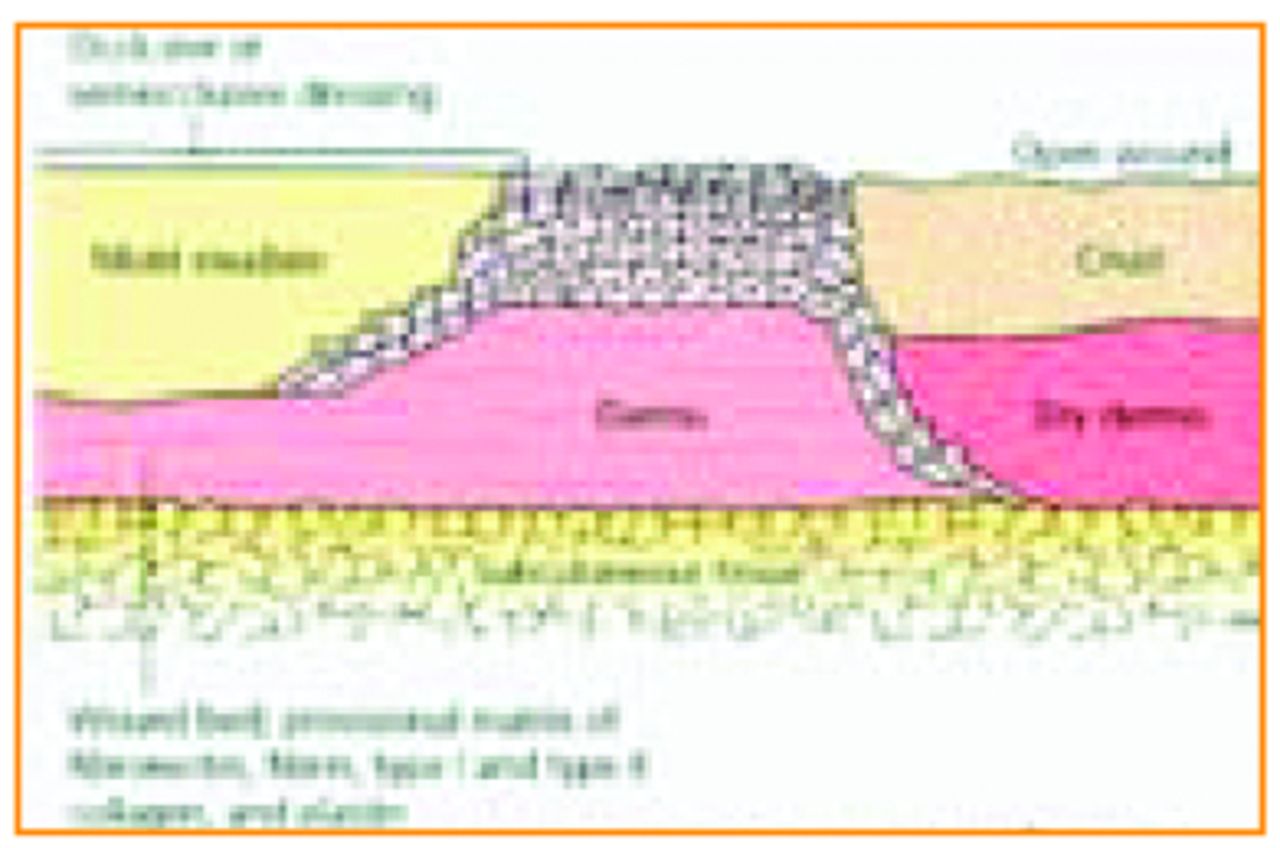
It is clear that for all wounds, achieving the optimal wound moisture balance is fundamental for optimal healing. Too wet and a wound gets macerated, too dry and reepithelialization is impeded and scar formation is encouraged (Figure 1).
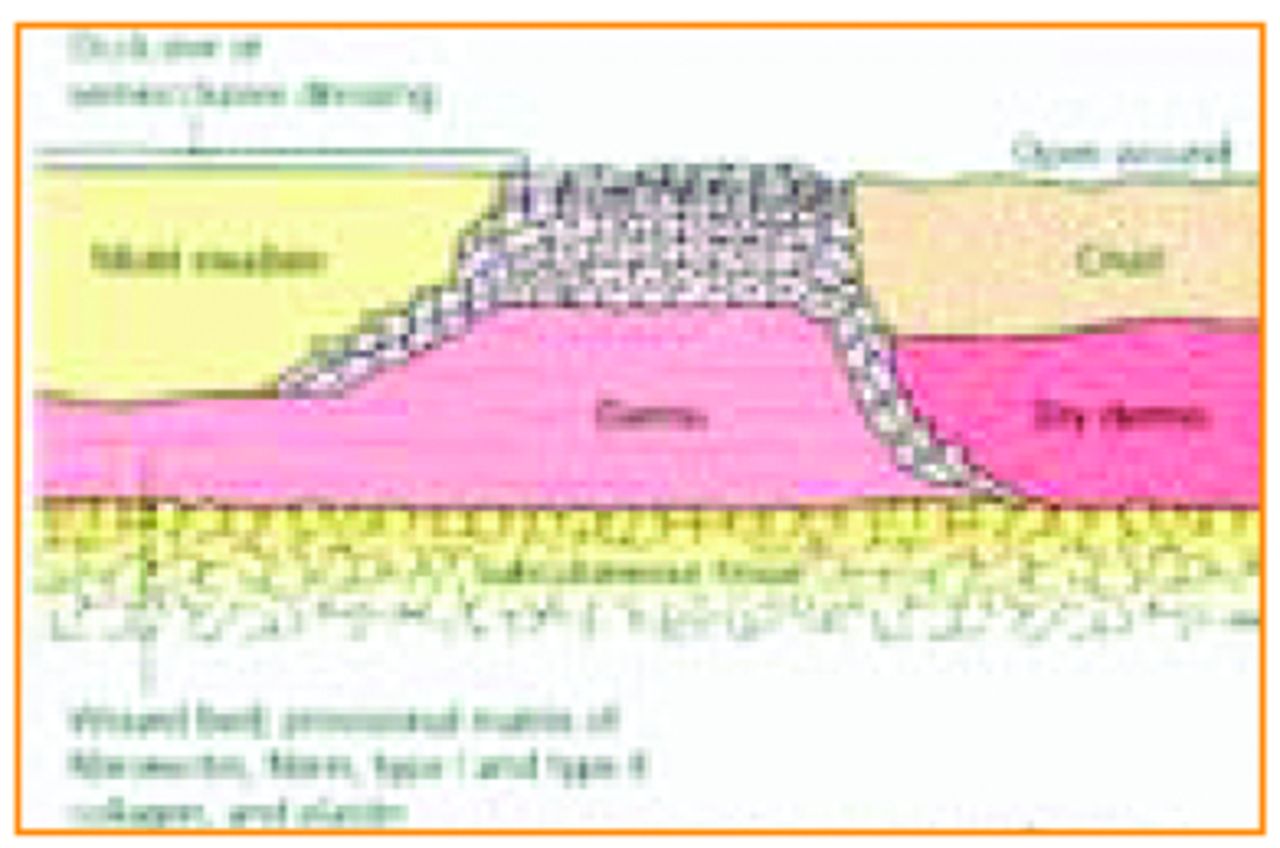
Occlusive dressing. The effects of tissue humidity on reepithelialization are shown. Occlusive dressings allow epithelialization to occur at the wound surface. In open wounds, the epithelium migrates beneath a desiccated crust and devitalized dermis. ©2010 Elsevier Inc. Habif: Clinical Dermatology, 5th Edition
Wounds for recipient sites, FUE, or traditional “strip” surgery are full-thickness wounds, and both granulation and contraction are a part of their healing process (Photo 1). It should be noted that trichophytic incisions are technically a partial-thickness wound with reepithelialization as the primary healing modality.
Full-thickness FUE wound.
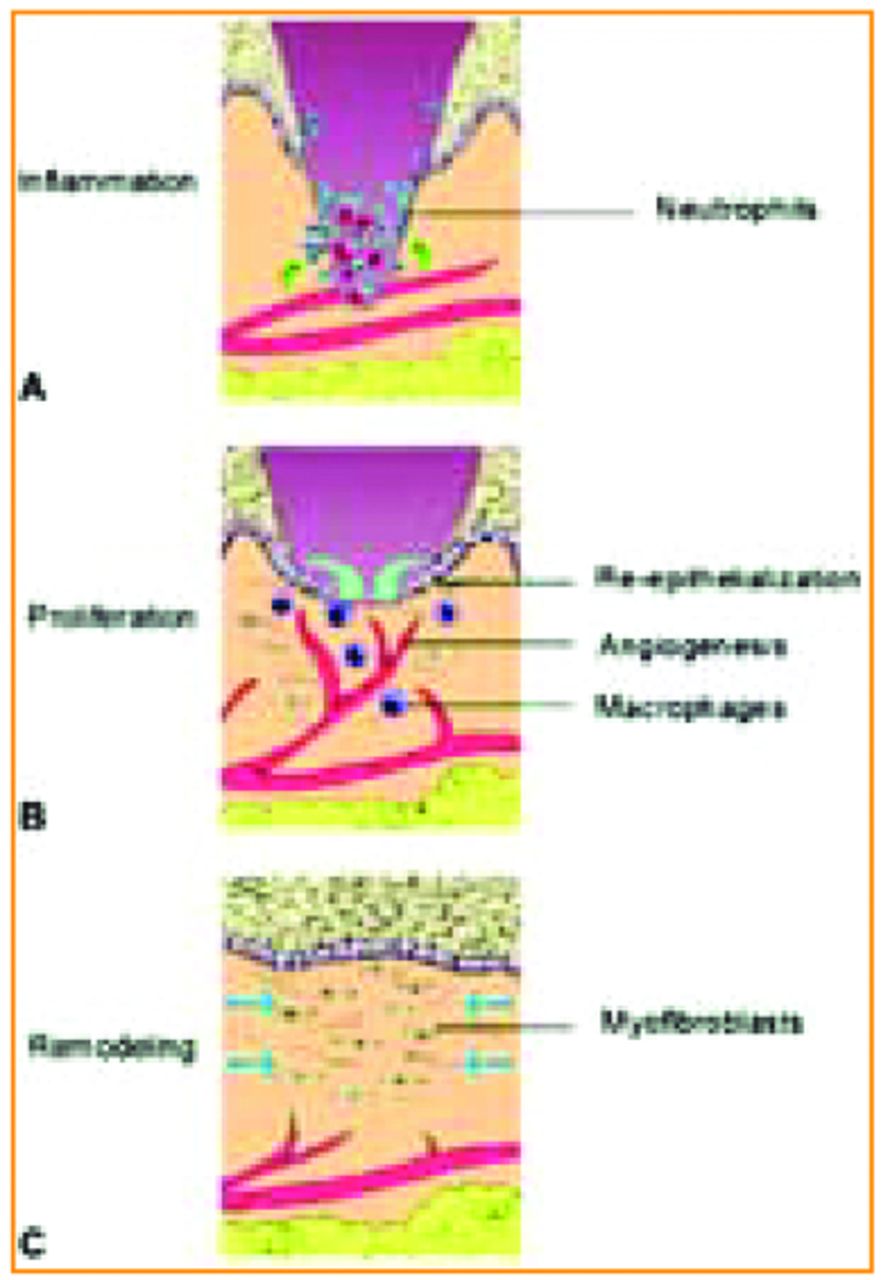
The acute period of wound healing lasts about 2 weeks and is divided into three phases. The inflammatory phase is the first and involves macrophage and neutrophil migration within the first 72 hours. Fibroblasts (and other inflammatory cells) will be activated by the damaged cells in the area. Vasodilation will permit these additional inflammatory cells to migrate to the area during this time, and fibroblasts will start to create the collagen structure. This means that from the moment the surgeon takes a strip or starts an FUE surgical process, the patient’s “wound healing” clock is ticking (Figure 2A).
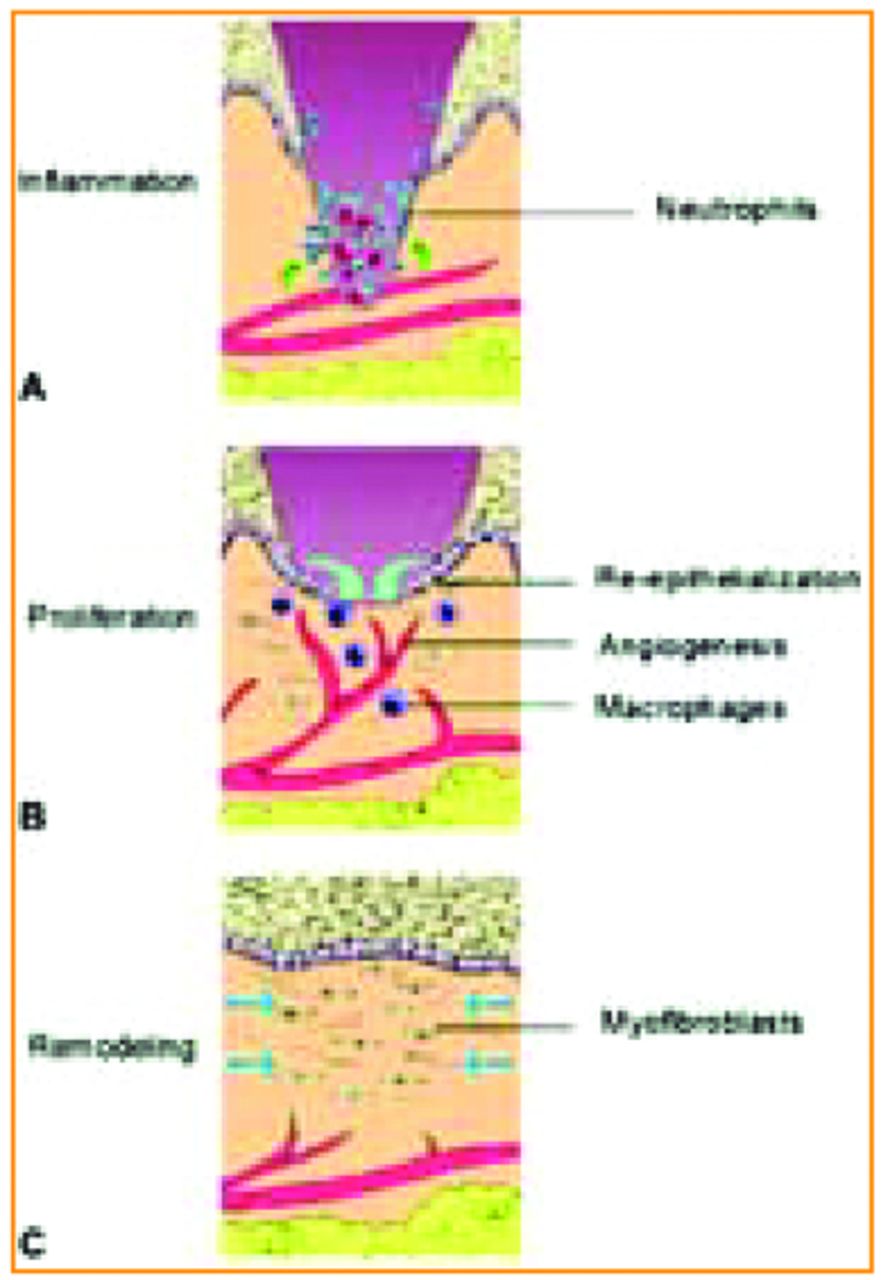
A: Inflammation; B: Proliferation; C: Remodeling. From Habif: Clinical Dermatology, 5th Edition.
The second stage is the proliferative phase and for a hair surgeon the majority of this phase occurs out of the office and out of direct control. Neutrophil numbers decline and fibroblasts and epidermal cells perform the majority of the wound healing processes including collagen matrix formation and closing of the wound itself. The matrix is an essential structural component, allowing the rest of the cells (keratinocytes and epithelial cells for instance) to migrate to where they are needed and then proliferate. This phase is where maintaining an adequate moisture balance (and occlusion if possible) is also essential because reepithelialization occurs fastest in moist, occluded wounds. Revascularization also occurs during this period (Figure 2B.)
The third and final stage is remodeling, which is characterized by fibroblast activity that re-works the collagen matrix over time and myofibroblasts that create wound contraction. This collagen matrix is particularly interesting, with new therapies to encourage its formation gaining popularity in many specialties (including ours—see ACell and PRP reports in previous Forum issues). Wounds will contract over the course of a full year and tensile strength increases over this period as well. While the strength is always less than 80% of normal skin, about 20% of this final strength will be generated within the first 2-3 weeks after the wound occurs.1 Thus, reducing the tension that a wound experiences during this time will prepare the patient for better healing in the future months (Photo 2; Figure 2C).

Scar post-trichophytic linear incision in remodeling phase.
Any discussion of wound healing in hair transplant surgery would be incomplete if it did not include a discussion of the importance of revascularization of the follicular unit. Revascularization of FUs occurs gradually and in several phases over the first week: plasmatic imbibition, primary inosculation, and secondary inosculation.2 Basically, the graft receives nutrients from plasma in the recipient site and after about 3 days begins to revascularize, completing this process by about day 7. The extent to which reperfusion injury occurs or how numbers and proximity of grafts influence final growth are open areas for debate and active research. It is likely that inter-patient variables account for the wide range of success (or failure) reported in the hair literature to date on these topics.
General Wound Healing Principles
Wounds created with a scalpel heal faster than those created by destructive means (laser or chemical cautery among them) so avoiding excessive tissue damage (such as with the use of tissue spreading) results in faster healing. Any foreign debris will slow wound healing by making the body do more work and possibly causing infection, so removing all spicules of hair and having high levels of vigilance with suture removal will improve outcomes.3 Keeping tension from the wound during healing is key to speedy recovery. There are several means that can be employed to minimize tension, chief among them being sub-cuticular sutures, avoiding lifting, and avoiding wide strip excisions where elasticity is low (Photos 3 and 4).4

Stretched scar.

Scar 1-year post-op. First surgery (TOP scar) done without sub-Q sutures. Second surgery (BOTTOM scar) done with sub-Q sutures.
Antibiotics help a wound to avoid infection better than antiseptics, and antiseptics like H2O2 can even slow wound healing.5 Occlusion speeds wound healing by speeding reepithelialization. Since occlusion is not always possible in hair-bearing tissues, a topical protectant to encourage reepithelialization is likely all that is needed. Elevation decreases swelling to the wound areas and thus speeds healing.
Donor Area Optimization
Wound healing in this area occurs on a longer time frame than the recipient zone since they are full thickness and require so much additional collagen formation and reepithelialization to close. Incisions made with a scalpel will heal faster than those made by more damaging methods. Additionally, avoiding any technique that causes tissue damage (e.g., electrocautery or wound cleansing with H2O2 solutions) will minimize resulting scars and wound healing times.1 Tissue-spreading techniques can also reduce healing times by lessening damage to individual follicles and thus avoiding problems like ingrown hairs or cyst formation.6
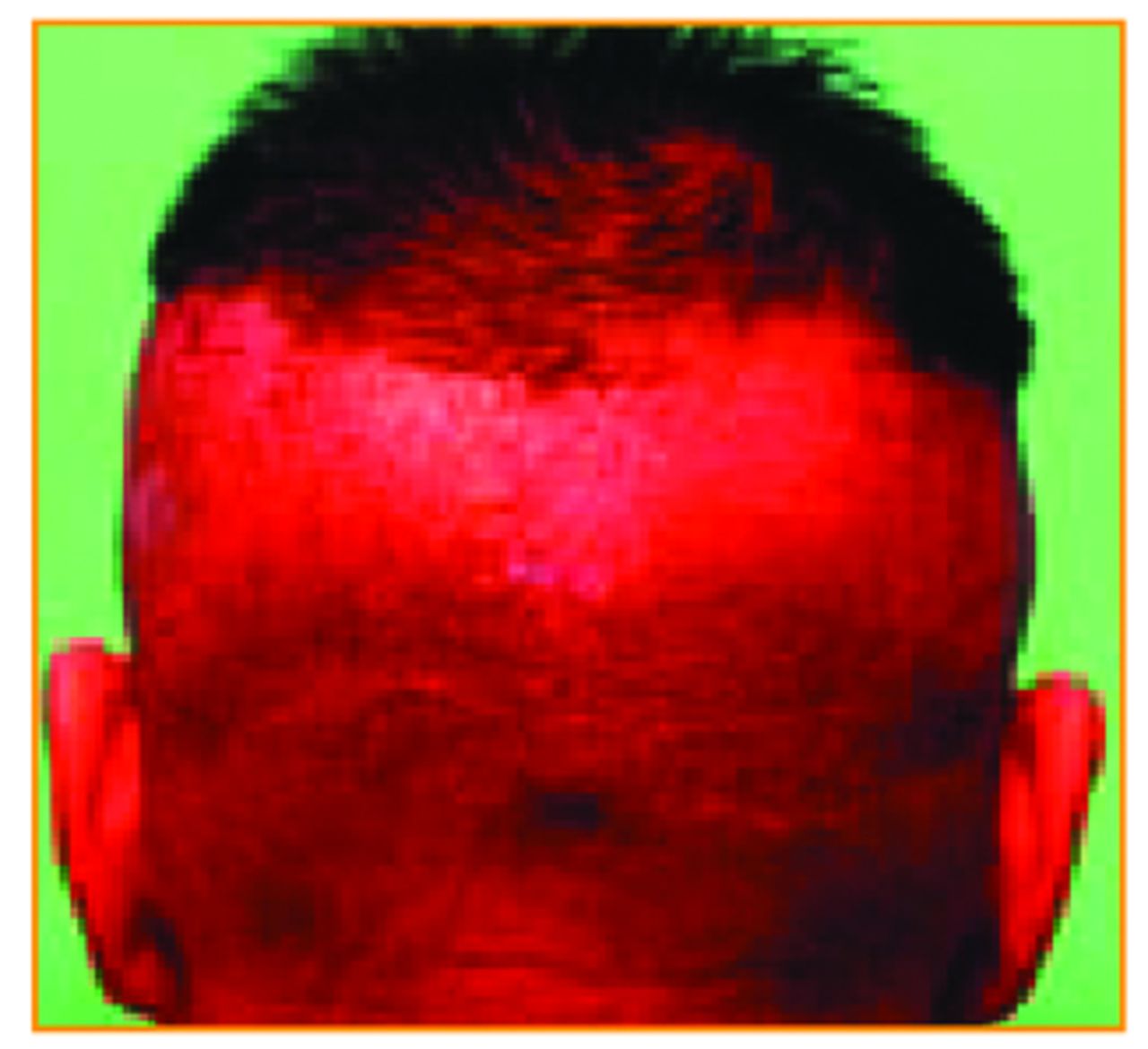
Assuming a trichophytic closure is used, healing in the donor area is a combination of both full-thickness and partial-thickness wounds. Therefore, occlusion with proper moisture balance would optimize the reepithelialization and reduction of tension reduces scarring. Full dressings would not encourage or speed wound healing of the modern hair transplant patient (although they were used with plug-type hair transplant surgeries). Unfortunately, the hair in the area prevents occlusion via conventional means (e.g., an occlusive dressing); therefore, an occlusive ointment is best (Photo 5).
Status post-FUE with occlusive ointment. An occlusive dressing could also be used.
Vaseline is adequate but, since it is petroleum-based, it may not be optimal. Prescriptions like Xenoderm, or emu oil can be useful. Remarkably, honey use has increased lately among wound care professionals and it seems to have immunostimulatory as well as occlusive properties (although no successful attempts to get post-operative hair transplant patients to put honey on their donor incision are known to this author).7,8
Whether the surgeon cares about the final appearance of his or her scar or not, reduction of tension via sub-Q sutures is important for any linear incision to minimize excessive collagen formation.9 Optimal wound healing in this area also involves adequate blood supply. In the majority of cases of scalp surgery, this is not an issue, but adjunctive therapies such as minoxidil and cold lasers can be used to possibly improve blood flow with good result.10,11 Cold laser treatments can be used the soonest while minoxidil should be avoided for at least the first week.12 Surgical preferences differ, but staples do have the advantage of producing less inflammation.13 However, for patients who wear their hair short, they can cause an undesirable “train-track” appearance with additional scarring in the form of a row of “dots” above and below the linear incision scar. Dissolving suture material such as Monocryl can worsen scar formation since these sutures require additional inflammation to be processed by the body, but they have an advantage for the patient since an additional suture removal visit does not need to be made. Nylon stitches seem to be the most comfortable for the patient (3-0 and 4-0) and do not induce excessive inflammation.
Recipient Area Optimization
Recipient sites typically heal faster than the donor area due to the small size of the incisions made, and so it is tempting to be less concerned about the wound healing in this area. However, this is the area that should be of chief concern to the hair surgeon, not least because of its visibility. Wounds in the recipient area are technically full thickness, but when the incision length is minimized on the scalp to less than 4mm, visibly “scarless” healing can be expected with minimal inflammation.
Due to the sheer number of wounds in this tiny area and the fact that the blood supply at the top and midline relies on diffusion at least partially, minimizing trauma to the vascular bed in order to preserve adequate blood supply is necessary. Damage to the vascular bed should be avoided by using minimal depth incisions and site-creating devices with the least tissue damage.
If no hairs exist in the recipient area at the time of transplant, it might be possible to use an occlusive dressing (again, NOT a full head dressing). If the patient tolerates this approach, the time frame for use would be the inflammatory and proliferative phases, about 3-5 days. Occlusion with an ointment has the potential to dislodge grafts if the ointment is viscous enough, or cause a local inflammatory reaction if products like Bacitracin are used (Neosporin seems not to induce much inflammation) (Photo 6).1

Inflammation in recipient area after Bacitracin and “BioOil” use.
The easiest approach might be to simply maintain moisture balance to encourage reepithelialization with showers or a frequent misting spray. For this purpose, straight saline or even water works well, although the commercially available copper peptide post-operative sprays can be used, too. Anything that dries the tissue, such as Rogaine® formulations containing alcohol (the 2% and 5% liquid forms contain 60% and 30% alcohol respectively) or sun exposure, should be avoided during this delicate time because it will prevent epithelial cell migration.
Grafts are also in a hypoxic state when they are transplanted and revascularization must occur for grafts to survive and grow robustly. Rogaine and cold laser treatments may be appropriate for use in the recipient area after the acute inflammatory and proliferative phases (about a week).12
Special Cases
FUE
Despite the small size of these incisions, it is clear from this investigator’s experience with tissue samples post-FUE that full-thickness healing takes place with full-depth scarring (Photo 7).

Note faint white scar tissue tracts from previous FUE.
Healing occurs much faster than in the sutured wound with many patients reporting about 3-5 days of active wound healing time until reepithelialization occurs. Since the scalp hair in the donor area is typically shaved short, this would be the perfect case to use an occlusive dressing if tolerated by the patient. The dressing would only have to be applied within the first few days to provide a substrate across which epithelial cells could migrate, but once the ~1mm wounds had closed, an occlusive ointment would preserve moisture balance in the area adequately.
Cyst formation and ingrown hairs can present a special long-term problem in FUE cases (Photo 8). Causes may vary from buried grafts to patient predilection for bacterial overgrowth on the head. Topical steroids or small Kenalog injections are appropriate in these cases since the addition of steroids, while known to slow wound healing, will not significantly alter outcome since these complications develop at a later stage. To that end, topical formulations should be used no longer than 2 weeks and Kenalog injections should be at a maximum dilution of 10mg/ml.

Post-FUE cyst formation.
Punch/Scars
Punch graft and/or scar revisions present a different problem since in these cases some scar tissue may remain in the area, slowing healing and making the final result more friable (Photo 9). Scar-to-scar or scar-to-healthy tissue healing occurs more slowly and thus allowances should be made for patients in this situation. Suture materials need to be kept in place longer and tension should be reduced as much as possible for up to 3 weeks to allow at least the acute phases of wound healing to be completed.

Punch graft scars.
Dense Packing/Mega-Sessions
Dense packing and mega-session techniques, while potentially more cosmetically beneficial, may suffer from the need for increased wound healing. For this reason, these techniques should be avoided by the novice surgeon and undertaken with caution and an eye toward careful patient selection if done by an expert. We are all cognizant that patient demands may push a surgeon to transplant graft numbers beyond the optimal limits of healing. In these cases, additional precautions should be taken to optimize both the donor and the recipient areas, including those discussed above. Possible additional measures include increasing the time away from exercise to minimize donor area tension, using staples and enforced occlusion wherever possible, and maintaining vigilant moisture balance.
General Principles for Optimal Wound Healing
So, short of handing them old lecture notes from medical school, what should we tell our patients? Patients always ask how they can optimize their wound healing, and while some of it is under their direct control, much of it is not. In fact, a large portion of a wound’s healing has to do with the inherent characteristics of the patient and the surgeon’s technique and surgical decision making. In general, it is wise to educate patients that some scarring will occur and no technique is completely “scarless.”
Moist wounds heal faster than dry open ones (many patients think it is the opposite).14 Malnutrition interferes with healing but mega-doses of vitamins (like Vitamin C or E) are unnecessary.15,16 Along these lines, zinc and copper are useful supplements for would healing, particularly in the inflammatory and proliferative phases since the collagen matrix is being deposited at that time, but in general these can be recommended with confidence. The copper peptide, commercially available as GraftCyte, may speed healing.17 Rogaine and laser treatments can be useful adjuncts to wound healing and graft re-growth (even if patients do not decide to continue with them long-term).11,12
In the final analysis, it is the experience and judgment of the surgeon that will result in a good outcome or avoid a poor one. Like it or not, the wound healing experiences of every hair transplant procedure a surgeon performs will reflect on his or her practice and on our medical specialty as a whole. Thus, we all owe it to each other and our patients to do everything in our power to produce optimal healing.
Editor’s note: After receiving Dr. Wasserbauer’s article, I sent out a poll on post-operative wound care to about 30 experienced surgeons to which I received 19 replies. The questions I asked included whether they kept donor and recipient areas wet, moist, or dry, and whether occlusive ointments and/or dressings were used. The results show that the majority keep both areas moist after surgery (see table), although it must be noted that the areas are often not kept continually moist. None kept the areas wet. Fewer respondents perform FUE so the numbers vary between the two types of operations. There was some variation in the type of solution used to keep the areas moist that included saline spray (most common), saline with ATP, and GraftCyte. The frequency and duration also varied from hourly to twice a day for anywhere from 24 hours to 2 weeks. Ointments were used commonly especially for the donor areas and included: Vaseline, Bacitracin, Copperpeptide gel, Aquaphor, Mupirocin, and Neosporin. Dressings when used include Vaseline gauze, GraftCyte, Saran wrap, Coban wrap, and Vigilon (hydrogel) with gauze and bandage. One respondent uses LLLT on patients who are able to come back for multiple visits. We are currently doing a study on post-operative use of the cold laser on wound healing and hope to have results for presentation in the Bahamas.
Although we know that moist wounds heal best, I have seen patients with excellent wound healing from surgeons who keep the areas mainly dry post-operatively. It would be interesting for someone to develop a clinical study looking at the different methods of post-operative care and assessing clinical outcomes. —NF
- Copyright © 2012 by The International Society of Hair Restoration Surgery
References:
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.