

Hair transplant surgeons are often faced with diagnostic uncertainty with regard to hair loss etiology. Patients presenting for surgical options may have scalp conditions that preclude surgery, and it is incumbent upon the surgeon to be able to properly diagnose these conditions. In addition to a careful history and examination of the scalp and hair shaft, it is helpful and often necessary to obtain a biopsy to assess histopathologic changes. Hair transplant surgeons without a dermatology background are often unsure about proper biopsy technique, and sometimes there are no convenient or willing dermatologists to see these patients. Therefore, to properly and more fully be considered an expert in hair loss, all scalp surgeons should be comfortable obtaining these specimens. The purpose of this article is to summarize the scalp biopsy technique to maximize diagnostic accuracy. Only a small subset of scalp conditions will be discussed, since mastery of the basic technique will allow specimen collection of virtually any disease process. An accompanying instructional video will be available in the near future in the ISHRS online Members Only Video Library.
Scalp conditions that usually require biopsy include all forms of scarring alopecia such as the following:
Chronic cutaneous lupus erythematosus
Lichen planopilaris
Frontal fibrosing alopecia
Graham-Little syndrome
Pseudopelade of Brocq
Central centrifugal cicatricial alopecia
Alopecia mucinosa
Keratosis follicularis spinulosa decalvans
Folliculitis decalvans
Dissecting cellulitis/folliculitis
Scalp conditions that infrequently require biopsy consist of non-scarring alopecias including telogen effluvium and alopecia areata. Scalp conditions that only rarely benefit from biopsy include hormone-mediated male and female pattern hair loss. In any patient where there is diagnostic uncertainty and where therapeutic options will be altered by an accurate diagnosis, a biopsy should be performed. One example is what would appear to be a non-scarring alopecia in a patient with lupus or lichen planus or other condition known to cause scarring hair loss. Another example is suspected trichotillomania where alopecia areata is a likely alternative.
The most important step in a scalp biopsy is determining the correct biopsy location. Selecting a site without diagnostic histologic features is a waste of time. The ideal site should be neither burnt out nor intensely inflamed. Captured tissue should include active inflammation if present and at least several hair follicles, and should generally be located at the periphery of an active area of hair loss.
Case 1
This 19-year-old girl presented to me with a diagnosis of discoid lupus on plaquinil therapy. She had presented to her primary care physician with new onset hair loss, and labs were obtained revealing an elevated ANA, triggering the diagnosis and treatment. My examination revealed a well-demarcated area of hair loss without evidence of scarring, but with inflammatory pustules (Figure 1). There were also numerous exclamation mark hairs, a diagnostic feature of alopecia areata. The history and atypical presentation warranted a biopsy. A biopsy site was selected at the periphery of the alopecic area, and included a pustule (Figure 2). A 4mm punch biopsy was obtained, and the wound was closed with 4-0 Nylon. Histopathology revealed the findings of a non-inflammatory alopecia consistent with alopecia areata. No features of lupus were seen. Based on these findings, a diagnosis of alopecia areata was made, the plaquinil was discontinued, and intralesional injections of triamcinolone were initiated. If necessary, immunohistology specimens would have been obtained.


Case 2
This 31-year-old Caucasian man presented with a long history of inflammatory hair loss treated with intralesional injections of triamcinolone. Examination revealed extensive patchy inflammation and follicular pustulosis (Figure 3). Figure 4 shows an example of a poor choice for a biopsy site. The extensive inflammation present might obscure important diagnostic features. Figure 5 shows a better biopsy site. Histopathology revealed the diagnostic features of folliculitis decalvans.



Case 3
This 50-year-old Caucasian woman presented with a many year history of slowly progressive frontal hair loss. There was no history of skin disease elsewhere on her body. Examination revealed evidence of scarring and perifollicular erythema (Figure 6). A biopsy site was selected near the periphery of the alopecic area and it included several inflamed follicular orifices. Histology revealed the findings of lichen planopilaris (LPP).

Case 4
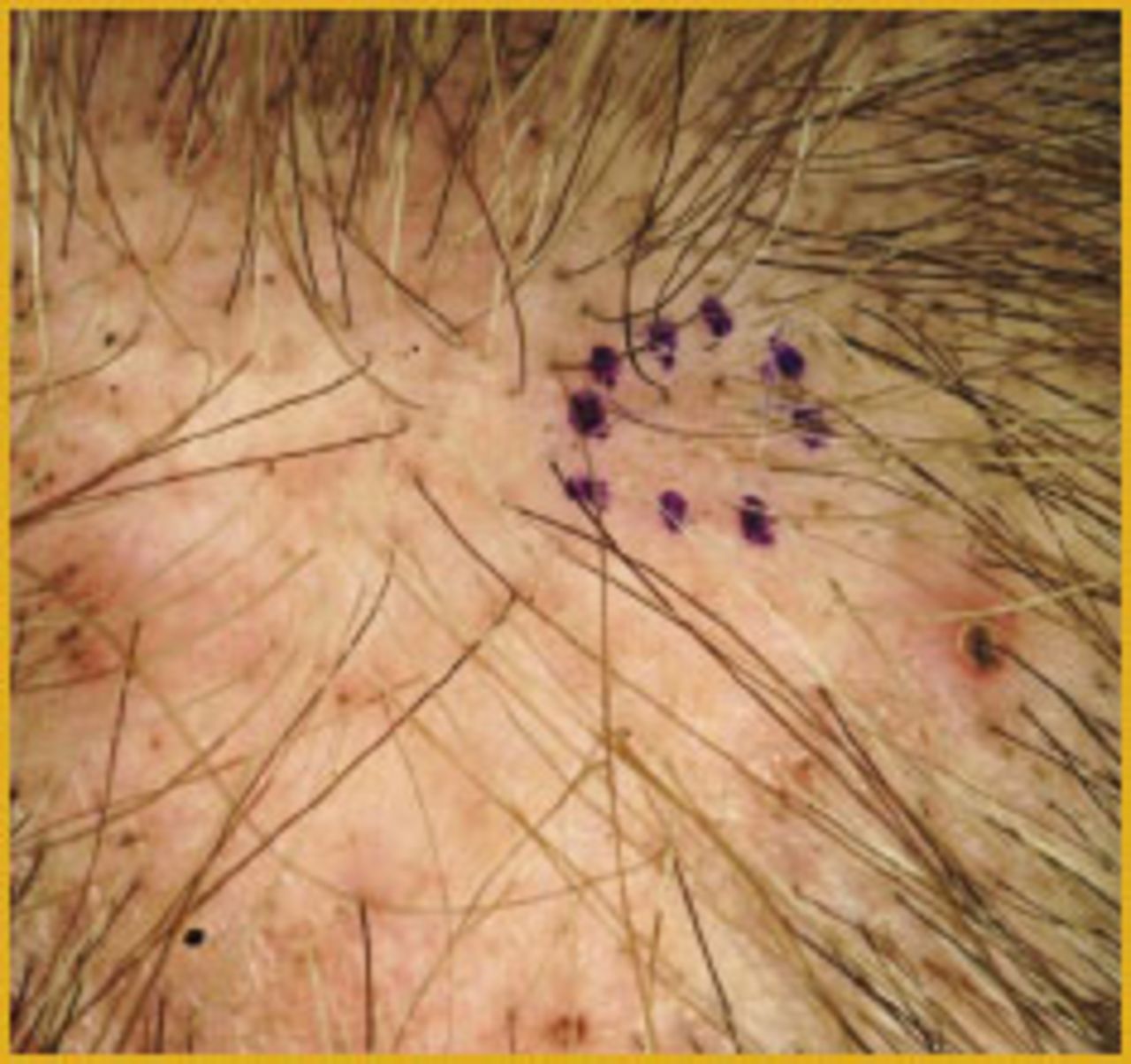
This 48-year-old Caucasian woman presented with a long history of facial papular mucinosis (Figure 7), and the more recent onset of hair loss involving the scalp and eyebrows. Examination revealed perifollicular erythema and scarring changes (Figure 8). The history and findings produced a differential diagnosis of alopecia mucinosis and LPP, and warranted a biopsy. In this case, a biopsy site was selected from the center of the affected area due to a cluster of affected follicles (Figure 9). A 4mm punch biopsy was obtained, with special stains revealing no mucin deposition, and with routine histology revealing the findings of LPP.


The biopsy technique itself is fairly straightforward. Required equipment includes a 4mm punch biopsy, sharp dissection scissors, forceps, and materials to place one or two sutures (Figure 10). After administration of local anesthetic (Figure 11), hairs to be captured in the punch are trimmed (Figure 12). The punch is angled parallel to the hair shaft direction to minimize hair shaft transection (Figure 13), and gently rotated until the blade has fully penetrated the scalp (Figure 14). Expect a lot of bleeding at this point due to the generous vascularity of the scalp (Figure 15). Using forceps, gently grasp and elevate the specimen (Figure 16). In some scalps, the specimen will separate easily from the underlying tissue without cutting. If necessary, using sharp dissection scissors, free the specimen from its deep dermal attachment. Close the wound with two interrupted 4-0 Nylon sutures or other closure of choice (Figure 17), and be prepared to hold pressure on this wound for a few additional minutes until bleeding has fully abated.









Most scalp conditions can be diagnosed with a single 4 mm punch specimen, which can be transected for processing in both vertical and horizontal orientations. At times, a second specimen may be required. Thus, working closely with your dermatopathologist is important to ensure that the desired specimens are submitted.
Mastering the punch biopsy technique is fairly trivial for a scalp surgeon, but it is crucial for proper patient care. Sending a patient to a dermatologist for a scalp biopsy can entail a delay of many months and the patient may incur significant expense. Handling this yourself will result in a speedier diagnosis and allow initiation of proper management more quickly.
- Copyright © 2013 by The International Society of Hair Restoration Surgery
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.