

My favorite non-scalp donor area is the beard. Beard hair can be used for a variety of applications to transplant the scalp with good results. Many patients will be able to provide 3,000-5,000 grafts from their beard region. I never try to remove all of the beard hairs, as I think having a thin beard looks more natural than having no beard. With every session, I harvest in an even pattern to maintain a well-distributed but sparser beard.
Harvesting can be challenging. There are typically whorls and significant variation in hair exit angle in the beard (Figure 1). There may be a dozen or more hair direction changes in a single square centimeter. Beard hairs exit the skin most obliquely along the jawline and submental region. The angle of emergence becomes progressively more acute on the submandibular region and neck as well as the face. It is essential in beard hair harvesting to recognize the blush of anagen hair as it passes through the epidermis (Figure 2). The lowest transection rates are achieved if the punch is centered on this blush rather than the hair shaft as it enters the skin. The technical keys to successful beard hair harvesting are using very sharp punches and shallow insertions—usually there is no need to go deeper than 2mm. Because of frequent angle changes, it is helpful to periodically lift and look to see the angle of the hair under the epidermis. Targeting anagen hairs identified by their growth after shaving and the blush produces the best harvest.

Whorls in the beard

Epidermal blush of telogen hair
The hypermobility of the beard area skin makes extraction difficult. It is critical to provide stretching and tensioning of the skin by having an assistant use two hands to create counter-traction; this is more important than tumescence. Tumescence to large areas is not effective as it disperses too rapidly. I prefer a two forceps extraction method: one to grasp the graft and the other to push the skin adjacent to the extraction site the opposite direction. Applying counter-traction during extraction helps to make extraction easier.
Anesthesia of the entire submandibular region of the beard can be achieved with a ring block (Figure 3). We use 4% articaine with 1:100,000 epinephrine diluted 3:1 with normal saline and then fill the field with 2% lidocaine with epinephrine 1:100,000 diluted 3:1 saline.

Ring block anesthesia
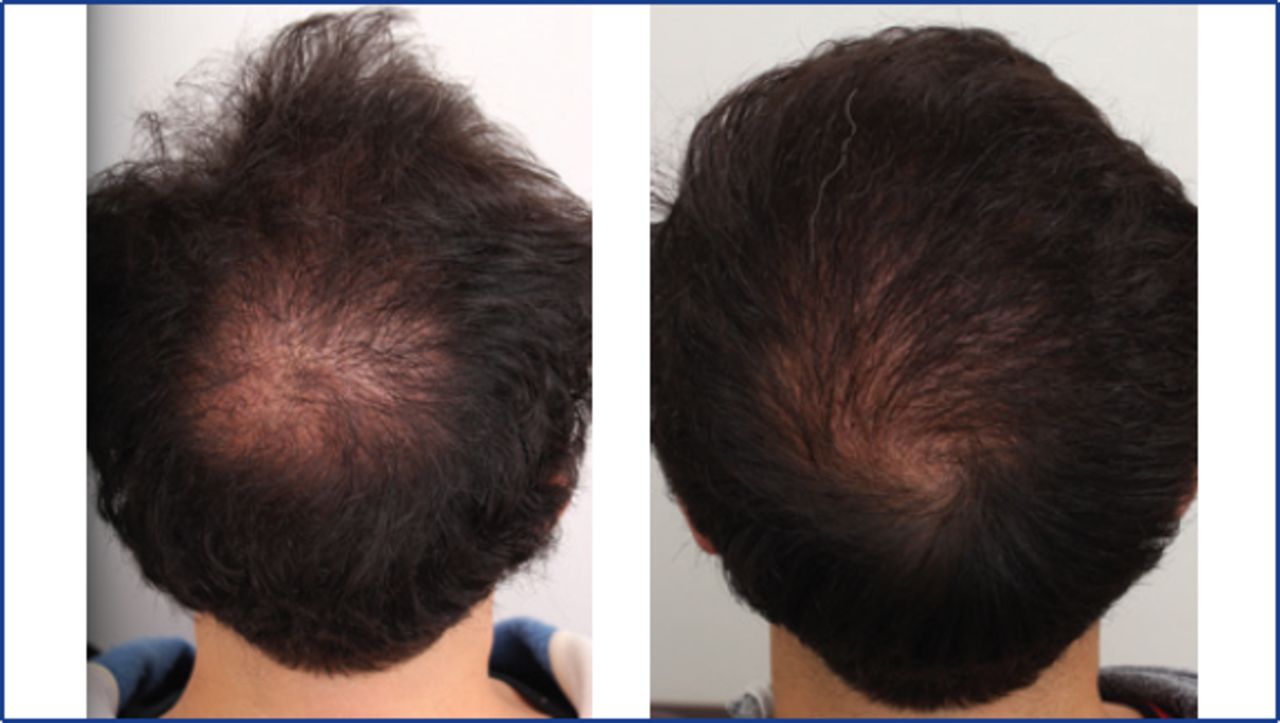
The survival rate of beard hair transplanted to the scalp is uniformly high and I am consistently impressed with how quickly it heals. I also find long-term healing is very good; it is very difficult to discern distinct scars or marks—the beard simply looks thinner as shown in Figure 4 after 2,450 grafts have been harvested. I don’t have a lot of experience with patients with dark complexions to know if this remains true for them, but my colleagues in India who perform a lot of beard hair extractions say darker skin also typically heals very well.

A: Beard area before extraction; B: beard area after extraction of 2,450 grafts; C: close-up of extracted beard.
I like beard best for donor scars (Figure 5).

Donor area scar before (left) and after (right) beard hair transplantation.
I think it is a good choice to add density for patients for whom you really want to preserve scalp donor supplies for later (Figure 6). Usually, beard hair is mixed among scalp hairs, but if scalp and beard hair texture is similar, beard hairs can be exclusively placed in scalp regions (Figure 7). Rarely would I use beard hair for the hairline, but patients with very coarse scalp hair are an exception.

Crown before (left) and after (right) beard hair transplant.

Crown before (left) and after (right) beard hair transplant.
Temporary partial facial paresis can occur in the beard area.
The motor branches of the facial nerve are located in areas we use for extraction. The marginal mandibular branch is most likely to be affected. Secondary to anesthesia and/or pressure on the nerve during extraction, patients may exhibit drooping of the mouth and lips. Typically, this resolves within 2-6 hours. As the nerve runs deep to the platysma, it is unlikely that it could be cut during surgery, but persistence of the paresis at 24 hours suggests that weeks may be required for resolution.
- Copyright © 2015 by The International Society of Hair Restoration Surgery
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.